Goodblend is Closing Its Dispensaries in PA
 Medical marijuana customers in Pennsylvania received some disappointing news when Goodblend PA, a subsidiary of Parallel Cannabis, announced the company was closing its operations in the state in order to serve “patients” in other more established markets. The Northside feed and grow operation is scheduled to close by September 15th 2023 and the dispensaries, located in Erie and on Baum Boulevard in Pittsburgh will close sometime in October. A planned dispensary in Cranberry Township will never open. Trib Live reported the company said in an emailed statement, “In connection with a strategic review, we have made the decision to withdraw from the Pennsylvania market in order to serve patients in our other, more established markets.” That could be good news for PA cannabis users in the long run.
Medical marijuana customers in Pennsylvania received some disappointing news when Goodblend PA, a subsidiary of Parallel Cannabis, announced the company was closing its operations in the state in order to serve “patients” in other more established markets. The Northside feed and grow operation is scheduled to close by September 15th 2023 and the dispensaries, located in Erie and on Baum Boulevard in Pittsburgh will close sometime in October. A planned dispensary in Cranberry Township will never open. Trib Live reported the company said in an emailed statement, “In connection with a strategic review, we have made the decision to withdraw from the Pennsylvania market in order to serve patients in our other, more established markets.” That could be good news for PA cannabis users in the long run.
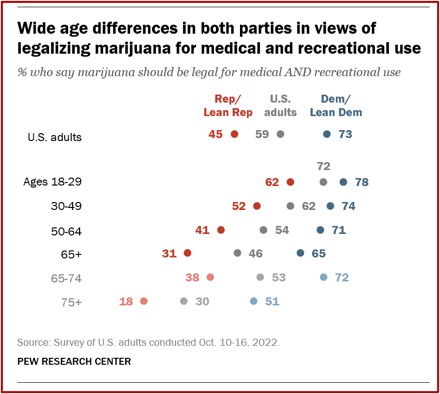
Medical marijuana was legalized in Pennsylvania is 2016 and dispensaries began to open in the state in 2018. According to the National Conference of State Legislators, as of April 24, 2023, 38 states have legalized cannabis products for medical use, and 22 states have legalized the recreational use of marijuana. But so far PA has resisted the pressure to join the 22 states who legalized recreational marijuana. I’d encourage the Commonwealth to continue to hold out while research related to the potential problems associated with marijuana use is completed and published.
In PREPARING to Legalize Cannabis, I reviewed two recent studies. One suggested cannabis use had strong associations with adverse mental health and life outcomes in teens. Another one added to the growing evidence of a causal association between cannabis use disorder (CUD) and schizophrenia that was said to be “almost certain.” Now a study published on August 29, 2023, in The Journal of the American Medical Association Network Open, by Lapham et al, found that CUD was commonly found among primary care patients in Washington State. Washington legalized recreational marijuana in 2012.
The New York Times reported that 21 percent of people in the Lapham et al study had some degree of a CUD. These findings were similar to previous research by Leung et al. They quantified the prevalence and risk of CUD as cannabis abuse (CA) or cannabis dependence (CD). Among people who used cannabis, 22% have CUD; 13% have CA (8-18%) and 13% (10-15%) have CD. The risk of developing cannabis dependence increased to 33% (22-44%) among young people who use marijuana weekly or daily.
Cannabis users need to be informed about the risks of developing CUDs and the higher risks among those who initiate early and use frequently during adolescence. Future studies are needed to examine how changes in cannabis policies may affect the risks of CUDs in the population.
The Lapham et al study in Washington State was conducted with data from Kaiser Permanente, a large health system in Washington. 5,000 patients 18 years and older were randomly selected from 108,950 eligible patients with a record of completing a cannabis screen as part of their routine primary care. They were categorized by their stated reason for using cannabis during the past 30 days: medical use only, nonmedical use only, or both. DSM-5 symptoms for CUD were used to assess severity, with 2-3 symptoms = mild, 4-5 symptoms = moderate, and 6-11 = severe.
Patients were asked about all modes of cannabis use as well as the primary mode, including inhalation (ie, smoke, vape, dab), ingestion (ie, eat, drink), application (ie, lotion, ointment), or other modes. Questions also included the frequency of past-year use and typical number of days per week and times per day of cannabis use.
Among cannabis users, 42.4% reported medical use only; 25.1% reported nonmedical use only; and 32.5% reported both recreational and medical use. The prevalence of CUD was 21.3% and interestingly did not differ depending of their reasons for use (i.e., medical use only). The most prevalent CUD symptoms for all groups were tolerance, uncontrolled escalation of use and craving. Patients with nonmedical use only or both reasons for use were more likely to report “withdrawal, use in hazardous situations, continued use despite consequences, time spent on use, interference with obligations, and activities given up.” Patients who reported any nonmedical use were at the greatest risk of moderate to severe CUD, with the lowest risk was among patients reporting medical use only. Lapham et al concluded:
In this study, CUD was common (21%) among primary care patients who use cannabis in a state with legal recreational use, with patients using for nonmedical reasons most at risk of moderate to severe CUD. As legal recreational cannabis use among adults continues to increase across the US, the results here underscore the importance of assessing patient cannabis use and CUD symptoms in medical settings.
So, as legal recreational marijuana use increases across the US, there is a corresponding call to assess people’s cannabis use and symptoms of CUD into standard medical care and practice. Research is also coalescing around a causative connection between using marijuana and schizophrenia. Teenaged use of marijuana leads to future adverse health and life outcomes. But there is a problem between the rapid pace of marijuana legalization and state and federal policy changes. These policy changes are happening faster than the scientific research can be done on the medical benefits and adverse consequences of marijuana.
In October of 2022 President Biden asked the Secretary of Health and Human Services (HHS) and the Attorney General to review how marijuana is scheduled under federal law. He also pardoned all people convicted of simple marijuana possession under federal law and urged governors to take similar action. Then on August 29th 2023 Politico reported the HHS Assistant Secretary wrote a letter to the DEA recommending that marijuana be moved from Schedule I to Schedule III. The letter is the last step in the official review process initiated by the President last October. Significantly, the DEA is not required to follow HHS’s recommendation.
The HHS recommendation was the result of an almost yearlong federal review of all available marijuana research. But advocates for the legalization of recreational marijuana and some lawmakers didn’t think the recommendation went far enough. They wanted the president to completely remove cannabis from the Controlled Substances Act. A cannabis advocate told Politico, “Rescheduling cannabis from 1 to 3 does not end criminalization.” However, if approved, the rescheduling would permit cannabis businesses to take tax exemptions for business expenses like salaries and benefits, providing a huge benefit to the financially struggling industry.
The shift in federal cannabis policy would also make it easier to conduct research on the health effects of cannabis consumption and for pharmaceutical companies to bring cannabis-based drugs to market. Researchers have long chafed at restrictions that only allow them to procure cannabis from a single farm at the University of Mississippi that bears little resemblance to the high-potency products many consumers are purchasing in state-legal markets.
Both legalization advocates and anti-legalization advocates are not happy with the HHS recommendation. Pro-marijuana advocates say it does not end criminalization, but anti-legalization advocates see it as potentially detrimental to public health. They say the “addiction profiteers” have been exposed for their lies about the physical, mental and financial benefits of legalization in the wake of the cumulating evidence of the harm being done to millions of Americans. “It is regrettable that the Department of Health and Human Services move now appears to be a nod to those monied interests.”
In August, ABC News did a short, 7-minute video in their Group Chat on how the increase in marijuana use could affect federal legislation, the economy, and national health, “How the legalization of recreational cannabis use is on the rise.” It’s available on YouTube, here. One of the individuals participating in this “Chat” said there is a lot of money at stake here in the marijuana industry. “It’s estimated that the marijuana industry can pump a hundred billion dollars into the overall economy this year.”
The health concerns were mentioned with a reference to a CDC report on its effect on teen health and wellbeing. “There are a lot of unknowns about the long-term risk of any cannabis exposure to developing brains.” According to the CDC marijuana use beginning in teen years or younger can affect brain development, which may impair thinking memory, and learning.” There were mental health issues, including schizophrenia. “The association between marijuana and schizophrenia is stronger in people who start using marijuana frequently at an early age.”
The health expert went on to say he hears from both sides is that “policy changes seem to be happening faster than scientific research. Now potentially rescheduling this from a class one substance can actually help with that research, but there’s a lot more we need to know.” But until then, we know already that several states are growing more cannabis than they can sell because there aren’t enough legal retailers in the market. The impact is that “the illegal marijuana trade is actually stronger and outpacing legal sales in states where it is legal.” In California, where recreational marijuana has been legal for seven years, unlicensed marijuana sales were more than double that of licensed sales.
Returning to Parallel Cannabis closing down its Goodblend facilities in Pennsylvania, there’s more to it than just wanting to serve “patients” in other more established markets. In the Green Market Report, John Schroyer reported the Atlanta-based company Parallel Cannabis is closing its three Goodblend PA facilities and leaving the Pennsylvania medical marijuana market because financial troubles led to a lawsuit from its landlord, Innovative Industrial Properties Inc. Pennsylvania is not the only state Parallel has had problems paying its rent. Parallel also defaulted on its rent for a facility in Texas. Parallel is one of the largest privately held multistate cannabis operators in the US, with additional facilities in Florida, Massachusetts, and Nevada.
Goodblend is struggling to get its own shareholders to agree to liquidate the business, with another pending lawsuit filed by Surterra Holdings, a division of Parallel. That suit alleges that minority owner Medical Bloom, which holds a 25% stake in Goodblend, has refused to agree to a dissolution. Parallel is asking for a court order to force the liquidation in order to pay off Goodblend’s debts, given that the Pennsylvania subsidiary is insolvent, the Post-Gazette reported.
So, in Pennsylvania, let’s not be seduced by the lure of money in legalizing recreational marijuana. The federal government is poised to reschedule marijuana, which will help the cannabis industry without removing marijuana from FDA oversight as a drug. Let’s wait a few more years and see what the scientific research tells us about the benefits and adverse effects from marijuana use before we begin to craft our legalization policy at the state or federal level. And let’s slow down the marijuana lobbyists at the state level who seem to be trying to get a preponderance of states to legalize recreational marijuana before that research has a chance to be done and published. If it means some more companies like Goodblend leave the state for more profitable fields elsewhere—or go bankrupt—good riddance.