Gambling with Cannabis and Psychosis

© Joshua Resnick | 123rf.com
Biological evidence supports a causal link between marijuana and psychosis. Additionally, this seems to be dose-dependent—with higher potency marijuana, there is an increased likelihood of a psychotic disorder. What is not clear, however, is whether at a population level patterns of cannabis use influence the levels of psychotic disorder. A new study published in The Lancet Psychiatry reported there is a strong link between high-potency marijuana and psychosis. “The odds of psychotic disorder among daily cannabis users were 3·2 times higher than for never users, whereas the odds among users of high potency cannabis were 1·6 times higher than for never users.”
If an individual began using marijuana before the age of fifteen, the odds were slightly increased, but not independent of the frequency of use or the potency of cannabis used. Compared with individuals who never used marijuana, those who used high-potency marijuana daily had four-times higher odds of psychosis. People who were using high-potency marijuana doubled their risk of psychotic disorder. “Our results show that in areas where daily use and use of high potency cannabis are more prevalent in the general population, there is an excess of cases of psychotic disorder.” The researchers estimated that 20% of the new cases of psychotic disorder could have been prevented if the daily use of cannabis had been arrested.
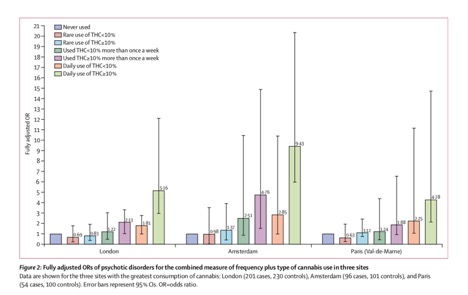
The study drew its data on first-episode psychosis cases from 17 areas in England, France, the Netherlands, Italy, Spain and Brazil. The novelty of this study was its multicenter structure and the availability of incidence rates for all the sites. The use of high-potency cannabis was a strong predictor of psychotic disorder in Amsterdam, London, and Paris where it was widely available. In the Netherlands the THC content can reach as high as 67%. See the chart below.
In conclusion, our findings confirm previous evidence of the harmful effect on mental health of daily use of cannabis, especially of highpotency types. Importantly, they indicate for the first time how cannabis use affects the incidence of psychotic disorder. Therefore, it is of public health importance to acknowledge alongside the potential medicinal properties of some cannabis constituents the potential adverse effects that are associated with daily cannabis use, especially of highpotency varieties.
Susan Gage, a psychologist and epidemiologist at the University of Liverpool, wrote a commentary on the study. Commenting for NPR, she said: “What this paper has done that’s really nice is they look at rates of psychosis and cannabis use in lots of different places where underlying rates of psychosis are different.” With regard to the finding that cities with more easily available high-THC marijuana have a higher rate of new diagnoses of psychosis, she said: “That’s a really interesting finding, and that’s not something anyone has done before.”
However, there are some who seek to minimize the findings. In “Psychosis is the last marijuana side effect you should be worried about,” on the Popular Science website, Kat Eschner not-so-subtly dismissed the findings as “an ableist morality fable,” comparing it to the film, Reefer Madness. For more on the film Reefer Madness, see “Remembering Reefer Madness.” She acknowledged that for a specific population of marijuana users, there was a link, but “overemphasizing the connection poses its own problems.” She quoted a University of York mental health and addiction researcher, Ian Hamilton, who pointed out the connection between cannabis and psychosis has been known for a long time and said: “I think we have to be careful we don’t exaggerate the risk.” But that was not all Hamilton had to say on the matter.
Hamilton published his own research into the association of cannabis and psychosis, in the journal Addiction. The University of York press release on his study indicated that while the population level risk of developing psychosis was low, and those vulnerable to developing serious mental health problems is relatively rare. But for individuals who already have schizophrenia, marijuana can make their symptoms worse. He said: “The research was clear that the more high potency cannabis used, the higher the risk of developing mental health problems, even if they are relatively low in number. For those who already had schizophrenia cannabis exacerbated the symptoms.”
Professor Robin Murray, a Scottish psychiatrist and Professor of Psychiatric Research at King’s College, London, “cautioned that cannabis is not as safe as was once thought.” In an editorial for the British Journal of Psychiatry, he said 10 of 13 longitudinal studies showed cannabis users are “at significant increased risk of subsequently developing psychotic symptoms or schizophrenia-like psychotic illness.” The remaining three studies showed a trend in the same direction. “A recent meta-analysis reported that the odds ratio for developing psychotic symptoms or a psychotic disorder in individuals who had used cannabis over non-users reached 3.9 (95% CI 2.84–5.34) among the heaviest users.”
He noted where most forms of cannabis in the 1960s and 1970s contained less than 4% of THC and an equal proportion of CBD (which ameliorates the psychoactive properties of THC). But these have been displaced by stronger varieties, which range in THC potency from 16% up to 90% as wax “dabs.” Then there is the rise of synthetic cannabinoids. “In contrast to THC which is a partial agonist at the cannabinoid CB1 receptor, most synthetic cannabinoids are full agonists and consequently more powerful.” He noted how “the USA and Canada have embarked on a major pharmaceutical experiment with the brains of their youth.” He suggested that the UK “wait and see the outcome of the experiment.”
Researchers at Radbound University published the results of a large-scale genetic study in Nature Neuroscience. “The researchers found that people with schizophrenia are also more likely to use cannabis.” There were 35 different genes associated with cannabis use, particularly with the gene CADM2. This gene was already associated with risky behavior, personality and alcohol use. They found a genetic overlap between cannabis and the risk of schizophrenia, which was no big surprise as other studies have shown the association of cannabis use and schizophrenia. However, they also showed a causal connection.
The researchers used an analysis technique called “Mendelian randomisation” to show a causal relationship between schizophrenia and an increased risk of cannabis use. This may indicate that people with schizophrenia use cannabis as a form of self-medication. However, the researchers cannot exclude a reverse cause-and-effect relationship, meaning that cannabis use could contribute to the risk of schizophrenia.
It seems that adolescents are at a greater risk of experiencing symptoms like hallucinations, paranoia and anxiety with marijuana use. Levy and Weitzman published a research letter in JAMA Pediatrics. They found that of 146 teen marijuana users, 40 (27%) reported hallucinations and 49 (34%) said they experience paranoia or anxiety. “Compared to youth who said they had only tried marijuana once or twice, adolescents who used it every month were more than three times more likely to experience hallucinations, paranoia or anxiety.” One in four reported symptoms of depression.
Adolescents with symptoms of depression were more than three times more likely to experience paranoia and anxiety. And they were 51% more likely to report hallucinations than teens without depression. Sharon Levy, one of the researchers said:
We don’t know if the greater exposure to marijuana over time made the brain more susceptible to psychotic symptoms, whether kids who experienced psychotic symptoms became more likely to continue to use marijuana or if some third factor, such as depression, made kids both more likely to use marijuana heavily and also more susceptible to psychotic symptoms triggered by marijuana. . . . Regardless of which of these explanations is most accurate, there is clearly an interaction between marijuana use and brain function.
A study published in The Journal of Child Psychology and Psychiatry found that increased use of cannabis between 13 and 16 was associated with a higher likelihood of having psychotic-like experiences (PLEs). The lead author of the study said: “Our findings confirm that becoming a more regular marijuana user during adolescence is, indeed, associated with a risk of psychotic symptoms.” Going from occasional use to weekly or daily use increased an adolescent’s risk of PLEs by 159%. Also see: “Psychosis and Adolescent Marijuana Use.”
It seems clear that as a society we are moving towards increased use and availability of marijuana. And where recreational marijuana has been legalized, there appears to be more potent forms of marijuana and an increasing incidence of psychosis. While a 1:20,000 risk of developing symptoms of psychosis is negligible, it won’t remain that rare as people play the odds with marijuana and psychosis.
This article was originally posted on 5/21/2019.