
In April, the CDC released another Health Alert update on the increasing risk for overdose with medetomidine. Known as ‘rhino tranq,’ ‘mede,’ or ‘dex,’ it is not approved for human use, but is approved for sedation in dogs. In humans, it can cause profound sedation, bradycardia (slow heart rate) and hypotension. It has been increasingly found as an adulterant with fentanyl, replacing its chemical cousin xylazine, known as ‘tranq.’ Reportedly, it’s 200 times stronger than xylazine.
The CDC said medetomidine was first identified in the drug supply in 2021 and began appearing in multiple cities that included Chicago, Philadelphia, and Pittsburgh from mid-2023 to mid-2024. “By late July 2024, medetomidine had been detected in drug samples and biological specimens from people who use illegal opioids in at least 18 states and the District of Columbia.”
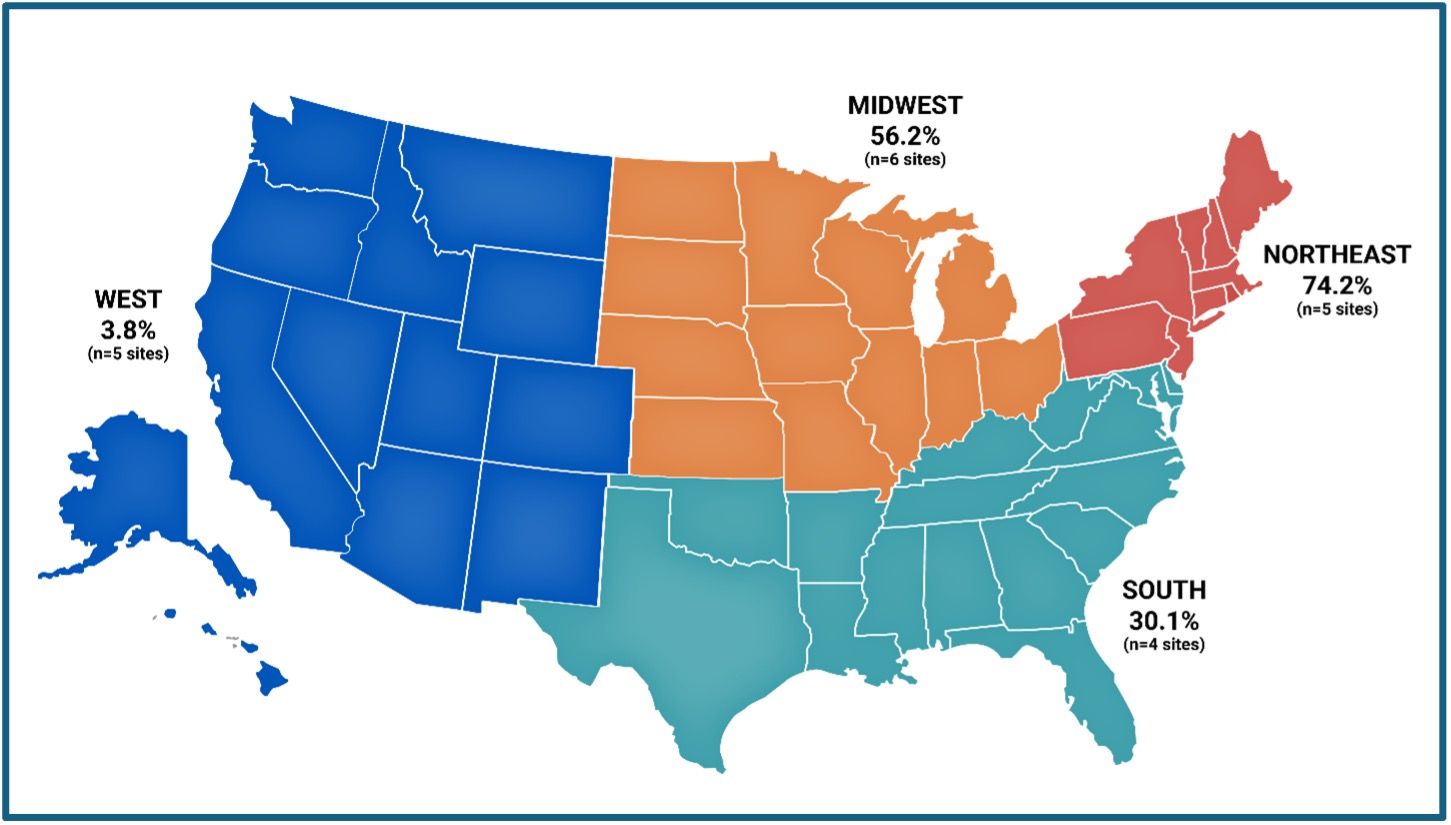
Reports on drug seizures by law enforcement submitted to the National Forensic Laboratory Information System (NFLIS) indicated medetomidine increased from 247 in 2023 to 2,616 in 2024 (950%), and then to 8,233 (another 215%) in 2025. The reports were concentrated in the Northeast (52%) and Midwest (31%), followed by the South (17%) and the West (<1%). Provisional data of the geographic spread and increased presence of medetomidine in illicit opioids from July 2025 to December 2025 is seen in the following map:
Unlike xylazine, medetomidine use does not appear to be associated with developing wounds. Similar to clonidine withdrawal, stopping medetomidine after regular use can require emergency or intensive medical care. Withdrawal symptoms are marked by tachycardia (above 100 beats per minute), severe hypertension, fluctuating alertness, tremor, chest pain, and uncontrollable vomiting. These symptoms can begin within hours of last use and peak 18-36 hours later. An emergency room physician and toxicologist with UPMC told the Pittsburgh Post-Gazette: “This is a life-threatening withdrawal syndrome.”
Complications such as non-ST elevation myocardial infarction and posterior reversible encephalopathy syndrome have been associated with severe medetomidine withdrawal. Increases in emergency department visits for non-alcohol, non-nicotine, and non-cannabis withdrawal have been temporally associated with medetomidine detection in the drug supply, with sustained prevalence linked to substantial emergency department and ICU utilization. From September 2024–January 2025, 165 patients across three Philadelphia health systems were hospitalized for fentanyl withdrawal complicated by severe autonomic dysfunction. Similar presentations were reported in Pittsburgh (October 2024-March 2025), where many patients required dexmedetomidine infusions and ICU-level care, and in Maryland (July 2025–August 2025), where medetomidine-related overdoses were frequently accompanied by withdrawal signs and symptoms.
Pittsburgh’s Experience with Medetomidine
Following the CDC Health Alert, the Pittsburgh Post-Gazette said medetomidine has been detected in the fentanyl supply in all corners of the U.S. Duplicating the above map originally in the CDC Health Alert, the Post-Gazette said the drug was detected in the Philadelphia drug supply in May of 2024 and then in Pittsburgh a few months later. Testing by the organization PA Groundhogs found medetomidine in 85% of the fentanyl samples from Pittsburgh, Philadelphia, and Trenton.
The associate medical director who is also an emergency department physician at Allegheny General Hospital said at first, they had no idea what was going on. “But now I feel like anytime there is a withdrawal, that’s what it is [medetomidine].” He went on to say he’d treated a man with a heart rate higher than 200 beats per minute. Most patients who come to the hospital in medetomidine withdrawal are admitted to the intensive care unit. Some experience lasting heart or brain damage.
During the snowstorm in late January, which brought a foot of snow to Pittsburgh, people weren’t able to access the drug supply, leading to a surge of withdrawal patients. An addiction medical specialist at the University of Pittsburgh said: “Their withdrawal symptoms came on very quickly, and they were ending up in the hospital.” Some days they had 10 to 20 at one hospital. The issue was straining intensive care unit capacity. ICUs weren’t designed with this population in mind.
He hoped the CDC Health Alert will be able to clue in physicians in other states before medetomidine overwhelms them; or an even stronger drug enters the drug supply. “Our goal is to try to accelerate that learning curve so when people see it, they know what they’re seeing, without having to go through the growing pains we did in Pittsburgh and Philadelphia.”
Although lawmakers have pushed for scheduling of both xylazine and medetomidine to curb supply, physicians and outreach workers worry it’s not a meaningful way to keep people safe from the volatile and ever-changing supply. They encourage consistent drug checking to inform both users and providers about the supply.
Pittsburgh now has access to medetomidine test strips, allowing users to check their supply before consuming it. Fentanyl and xylazine test strips are also available and distributed to patients. Pennsylvania has been doing a better job in responding to the problems with medetomidine, but a physician and professor of addiction medicine at the University of Pittsburgh was worried about now that the CDC has released the alert, what will happen at the public health level.
Public health needs to learn from some of the patterns we’ve seen before, and policymakers need … to realize that scheduling doesn’t necessarily mitigate risk, and criminalization of patients isn’t going to be beneficial for their health.
Medetomidine Emerges in New York State
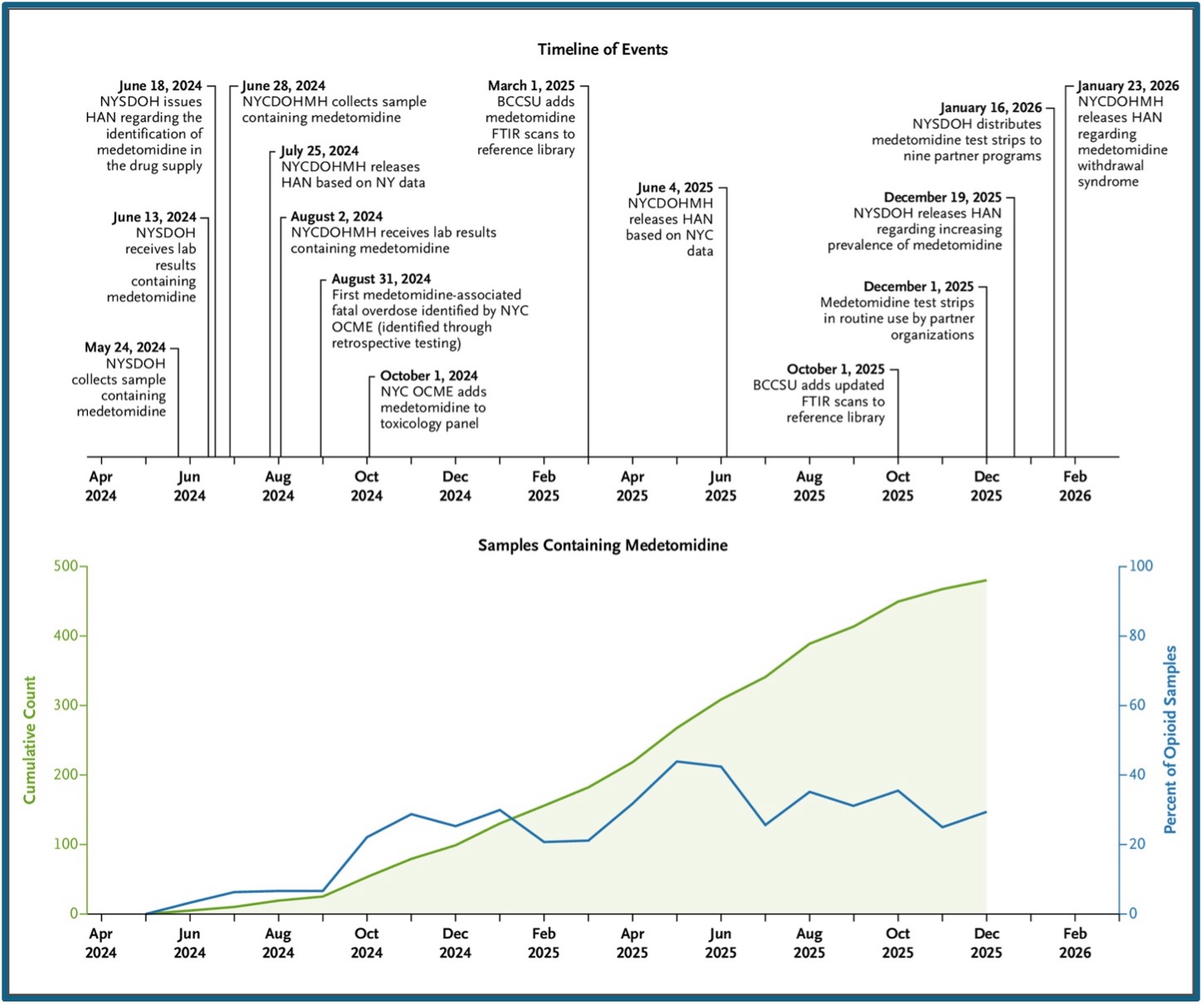
The New England Journal of Medicine published “Emergence of Medetomidine in New York’s Illicit Drug Supply” in April of 2026. The report highlighted state and local collaboration in New York state to detect emerging substances of concern in the illicit drug supply and then implement data-guided responses. Medetomidine was first detected in New York on May 24, 2024 in a sample collected in an upstate county, which produced unexpected sedative effects. In June of 2024, additional samples containing medetomidine were collected which were involved in two nonfatal overdoses. The first recorded overdose death in which medetomidine was seen as a contributing factor occurred in August of 2024.
Drug-checking technicians were routinely using medetomidine test strips by December of 2024. After months of laboratory detection in less than 10% of opioid samples, medetomidine increased in the illicit drug supply with an abrupt and sustained increase to over 20% of collected opioid samples by October of 2024. From May of 2024 through December 2025, 25.1% of total included opioid samples contained medetomidine. See the following figure.
Abbreviations used in the figure are as follows: BCCSU denotes British Columbia Centre on Substance Use; FTIR, Fourier-transform infrared spectroscopy; HAN, Health Alert Network; NY, New York; NYSDOH, New York State Department of Health; NYCDOHMH, New York City Department of Health and Mental Hygiene; and OCME, Office of Chief Medical Examiner.
The Times Union, serving the Capitol Region of New York, said the findings of the research in “Emergence of Medetomidine in New York’s Illicit Drug Supply” offer the clearest picture of how fast a new adulterant can take over a street drug market. One of the co-author’s of the study acknowledged the data cannot explain why medetomidine spread so quickly, only that it did. “We may not always know exactly the cause, why it has increased so much, but the first thing that we need to be able to do is to identify these trends.”
He thought the deeper question was whether New York could catch the next unknown substance earlier than it caught this one. “Every overdose is too many. When we see the numbers moving like that from one year to the other, it really tells us this is a time-sensitive issue.” The opioid problem seems to be accelerating.
Heroin ruled the illicit opioid market for several decades, until fentanyl began to spread in 2014 and became the dominant opioid. Xylazine arrived as an opioid adulterant in the early 2000s and by October of 2022 was present throughout the U.S. Medetomidine first infiltrated the illegal drug supply in 2021 and began appearing with fentanyl in multiple jurisdictions that included Chicago, Philadelphia and Pittsburgh from mid-2023. By late July of 2024 medetomidine was detected in illegal opioids in at least 18 states and the District of Columbia. By 2025 medetomidine was present throughout the U.S. (see the map above).
God help us be prepared for the next incursion into the illicit opioid market. For other articles on medetomidine, see “Medetomidine and Illicit Opioids” or “A New Adulterant for Opioids Called ‘Flysky.‘”



