
A study published in the Canadian Medical Journal found that ADHD diagnoses increased over the last twenty years, particularly after the pandemic began. They found a sevenfold rise in the rate of new recipients of prescription stimulants among adults in Ontario since the start of the pandemic. Medpage Today noted that some of the sharpest post-pandemic increases were among teenage girls and young women. Experts suggested the increase may be due to the diagnostic changes introduced in 2013 with the DSM-5 and improved awareness, but they also warned of potential misdiagnosis from pandemic distress.
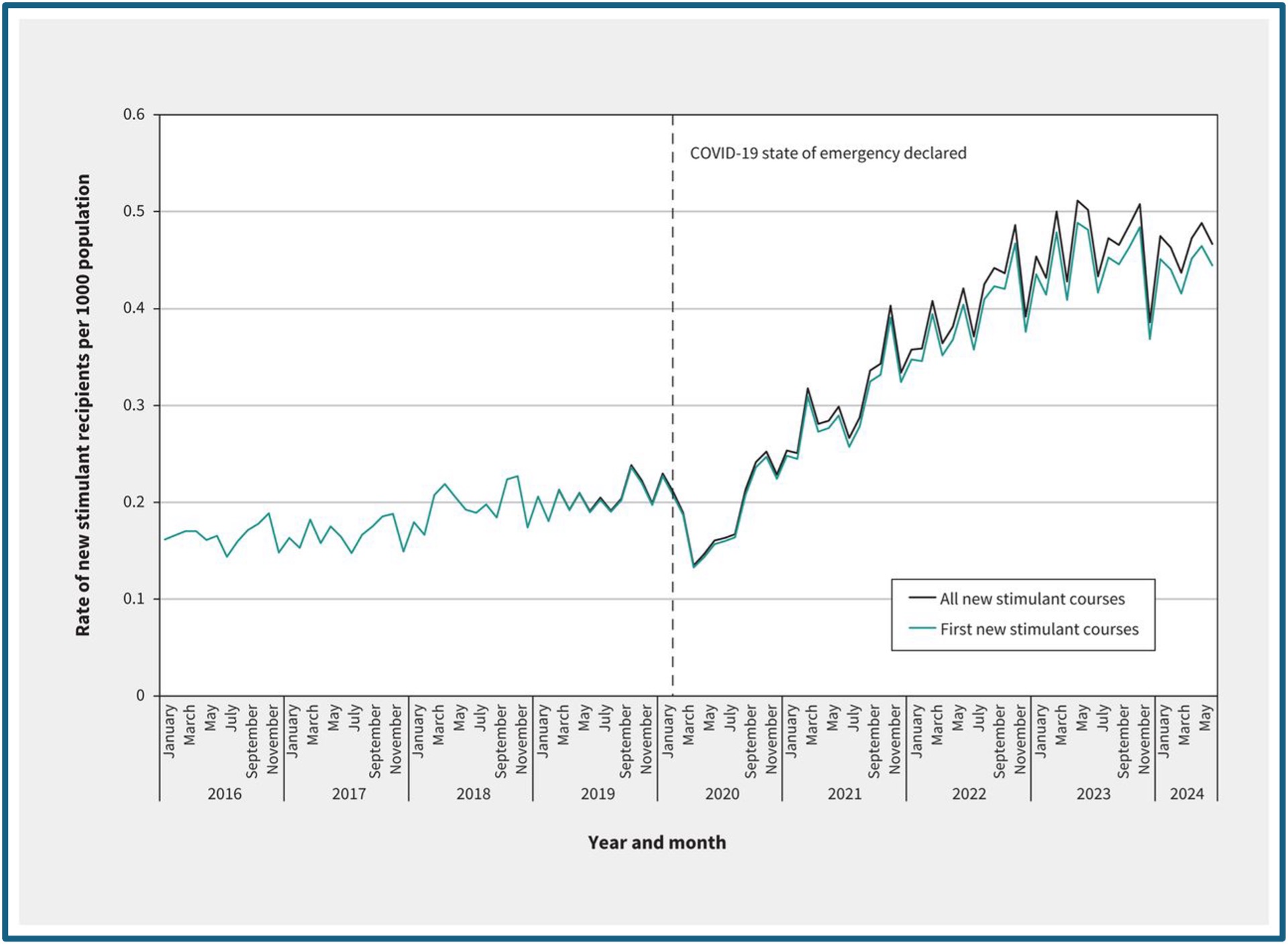
The Canadian researchers said their results may indicate improved recognition and treatment of adult ADHD, but also raised concerns about potential overdiagnosis and overtreatment of ADHD. “Notably, females were disproportionately affected, with initiation rates surpassing those of males across nearly all age groups at the end of the study period.” They also observed temporal changes in prescribing, with fewer prescriptions initiated by psychiatrists and more prescribed by primary care providers and nurse practitioners; and the role of virtual visits that began during the COVID-19 pandemic. See the following figure from the study.
In the United States, the rate of stimulant prescribing for adults has been increasing, with similar upward trends documents in Australia, the United Kingdom, and Finland. The findings reflect global trends in stimulant prescribing in postpandemic times, which could be the result of improved access to care and greater awareness of adult ADHD. “However, other potential factors — including the influence of social media, long COVID, and transitions to telemedicine platforms — may also be contributing to rising demand.”
Rising awareness of ADHD through social media in this period may have also driven some to seek formal diagnosis or stimulant treatment, although this potential influence requires further empirical investigation. Finally, more than one-quarter of people newly starting stimulants appeared to have a diagnosis of anxiety or depression, with the absolute number of people with this diagnosis nearly doubling during the pandemic. Therefore, some of the observed trends may have been associated with the use of stimulants as an adjunctive treatment for major depression.
These findings may partly reflect improvements in access to ADHD treatment and diagnosis during the pandemic, but they also raise questions about the quality and appropriateness of stimulant prescribing for adult ADHD. The researchers observed a shorter interval from the first ADHD-related health care visit to beginning stimulants during the pandemic. Additionally, they noted the growing involvement of nonspecialist prescribers (i.e., primary care providers and nurse practitioners) and online services where access to specialist assessment is limited.
This raises broader concerns about the risk of misdiagnosis and inappropriate stimulant prescribing in the absence of sufficient time, support, and diagnostic resources. Importantly, high-quality adult ADHD diagnosis requires adequate clinical time and access to appropriate expertise; resources that are often constrained in routine care. The relatively low proportion of people with an ADHD-related health care interaction, despite rising prescription rates, underscores the need for more rigorous assessment protocols and better alignment between diagnosis and treatment. Improvements in accessing expanded mental health care and specialized psychiatric services are critical to lowering the threshold for diagnosis and treatment, particularly for conditions like ADHD, which can persist into adulthood. Missed diagnoses in childhood may contribute to legitimate new diagnoses later in life, and rising stimulant prescriptions may reflect efforts to address these historical gaps in care, particularly among females. However, this trend must be balanced against the risks of overprescribing and misdiagnosis, particularly in the context of limited oversight in some telehealth and nonspecialist prescribing environments.
One of the researchers told the Independent many of the findings were consistent with trends in global stimulant prescribing in the post-pandemic era, and are likely influenced by greater awareness of adult ADHD and improved access to care. “However, the rising impact of social media influencers on ADHD awareness in young adults, as well as the rapid evolution of virtual health services that support online assessments and treatment, may also be contributing to misdiagnoses and potential harm.”
A study published in the Lancet Regional Health Europe in 2026 found the use of medication to treat ADHD had increased dramatically among adults, more than a 20-fold increase in females and 15-fold increase in males. Some experts thought the findings showed an increasing number of people with ADHD were seeking help, while others suggested the rise was a worrying sign that too many people were being put on drugs. The researchers analyzed electronic health records from Belgium, Germany, the Netherlands, Spain and the UK.
Problems with Adult ADHD
Prophetically, Allen Frances warned in his 2013 book, Saving Normal, that the DSM-5 set the stage for creating a new epidemic of ADHD in adults. Frances was the chairman of the DSM-IV Task Force and part of the leadership group for DSM-III and DSM-III-TR. He pointed out where attention problems and restlessness are nonspecific and extremely common among normal adults and those suffering from various other mental disorders.
The easy path to adult ADHD suggested by DSM-5 will mislabel many normal people who are dissatisfied with their ability to concentrate and get their work done, especially when they feel bored and don’t like the work they’re doing. It will also misdiagnose those whose problem in concentrating is really caused by something else—e.g., substance abuse, bipolar disorder, depression, all the anxiety disorders, OCD, autistic disorders, psychotic disorders, and many others. No one should ever get diagnosed or treated for adult ADHD until all of these are first ruled out as the primary cause—lest inappropriate stimulant treatment may worsen their already existing psychiatric problems.
Frances went on to say adult ADD was already, in 2013, too easily diagnosed. Symptoms were mostly subjective, based on fallible self-perceptions of poor concentration and task accomplishment. “The DSM-5 lowering of requirements will capture many adults who want to be sharper but don’t have specific or serious enough problems to qualify for a mental disorder.” He predicted “fake adult ADHD” would be common in college students, people with demanding jobs, and those who struggle to stay awake, like long-haul truck drivers.
He said the wider distribution of stimulants was simply too important a public health and public policy issue to be decided by a small group of DSM-5 experts “who are focused on their own narrow diagnostic question.” He had no opinion on whether stimulant use should be allowed for performance enhancement. “But I am strongly opposed to lowering the criteria for adult ADHD in a way that indirectly promotes their fake ‘medical’ use in those who don’t really have a mental disorder.” Difficulties meeting societal expectations should not all be labeled as mental disorders.
The criteria for a first-time diagnosis of ADHD in adults should be more, not less, rigorous. In evaluating any given adult for ADHD, we must be sure that all the many psychiatric causes of inattention are first ruled out and that the problems are a continuation of ADHD symptoms that started in early childhood. Any late onset of attentional problems is caused by something else, not ADHD. Let’s keep DSM as a manual of mental disorders and not turn it into a vehicle for performance enhancement.
Frances’ predictions about the fallout from lowering the diagnostic requirements for ADHD in the DSM-5 is evident in the above figure, where you can see a gradual increase in from 2016 to 2000. But then after the COVID pandemic began, the floodgates were opened; ADHD diagnosis and stimulant prescriptions accelerated even more. Improved access to care and greater awareness of adult ADHD were not the only contributing factors to that increase.
ADHD research has continued and there have been two new interesting developments. One has to do with the heterogeneity of ADHD, and another study discovered that stimulant medications don’t “treat” ADHD way we’ve thought they did.
Types and Treatment of ADHD
In the journal Cell, Kay et al published, “Stimulant medications affect arousal and reward, not attention networks.” For decades, the medical consensus has been that stimulants like methylphenidate (Ritalin, Concerta) treat ADHD by targeting regions of the brain that control attention. But the study showed prescription stimulants worked by making individuals more alert and interested in tasks, rather than improving their ability to focus. A press release from WashingtonU Medicine said rather than activating the attention centers of a child with ADHD, stimulant drugs work by making activities the child normally struggled with feel more rewarding.
These results also provide a potential explanation for how stimulants treat hyperactivity, which previously seemed paradoxical… Whatever kids can’t focus on—those tasks that make them fidgety—are tasks that they find unrewarding. On a stimulant, they can sit still better because they’re not getting up to find something better to do.
PsyPost said to verify these findings, the research team conducted a separate validation study with five adults who did not have attention deficits. They underwent repeated brain scans before and after taking a controlled dose of methylphenidate. The results mirrored the findings in the children. “The medication consistently altered the arousal and reward networks while leaving the attention networks largely unchanged.”
By shifting the focus from attention to arousal and reward, this research fundamentally alters the understanding of how psychostimulants function. It suggests that these drugs are not “smart pills” that boost intelligence. Instead, they are endurance tools that help the brain maintain effort and wakefulness in the face of boredom or fatigue.
Not only does this research alter our understanding of how psychostimulants function but seems to imply the label ADHD—Attention-deficit/hyperactivity disorder—does not adequately name this disorder. Either that, or psychostimulants aren’t an appropriate treatment because they don’t change attention networks in the brain.
In JAMA Psychiatry, a study by Pan et al said while ADHD symptoms are portioned into inattentive and hyperactive/impulsive domains, this binary behavioral classification can’t capture the complexity of ADHD. Clinical observations revealed diverse patterns cutting across the DSM-defined domains. They thought the consensus-based distinctions within the DSM perhaps oversimplified the neurobiological mechanisms underlying ADHD. And this posed a major challenge in the diagnosis and treatment of ADHD.
The three main subtypes of ADHD described by the American Psychiatric Association are: 1) predominantly inattentive, 2) predominantly hyperactive/impulsive, and 3) combined. Instead of starting with these DSM-defined domains, Pan et al began with a brain-first approach that provided biological validation of the identified subtypes through data-driven clustering. They found three distinct biotypes with unique clinical-neural profiles. See the JAMA Psychiatry article for a more comprehensive discussion of their methodology and results.
The researchers thought their study advanced the understanding of ADHD heterogeneity. “The replication of our findings across 2 cohorts suggests that our approach may offer a feasible framework for stratifying ADHD cases.” They thought while DSM classifications relied on consensus-derived symptoms, their neuroimaging-derived clusters converged with clinical phenotypes without using any clinical features. “This convergence provides compelling evidence that these presentations reflect genuine neurobiological entities, biologically validating these long-observed clinical distinctions.”
As always, further research to replicate and confirm these findings with ADHD heterogeneity and psychostimulant treatment of ADHD needs to occur. But it does seem ultimately, that the ADHD diagnosis in the DSM is in for some future changes.



