
In 2016, the DEA announced its intention to place kratom and its active ingredients, mitragynine and 7-hydroxymitragynine (7-OH) into Schedule I of the Controlled Substances Act, making it an illegal substance like heroin and marijuana. There was a wave of protests from kratom users and advocates and the DEA rescinded its intent to classify kratom in October of 2016, which meant it has remained unregulated since then. But a new study by the CDC found the number of kratom-related exposure reports by poison centers increased 1,231% from 2015 to 2025.
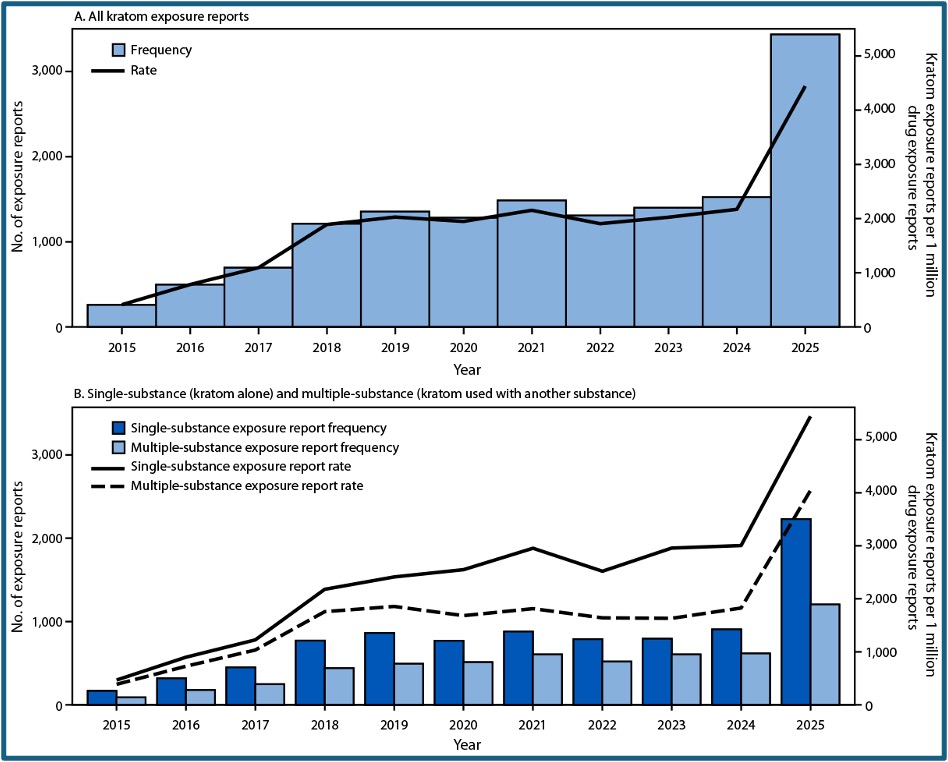
During the 2015-2025 time-period, US poison centers documented 14,449 kratom exposures. There was a steady increase of reported exposures through 2019, followed by a plateau during 2020-2024. Then in 2025, there was a marked surge of exposures with 3,434 kratom exposures. Kratom only (single substance reports) accounted for 62% of all kratom reports and multiple substances accounted for 38% of all kratom-associated reports.
“The most common substances involved in multiple-substance exposure reports across this study period were addictive substances (ethanol, 22%; opioids, 16%; benzodiazepines, 15%; cannabis and cannabinoids, 12%; and stimulants, 11%) and antidepressants (14%).” Interestingly, the large increase in 2025 coincides with the emergence of high-potency, semisynthetic kratom formulations like 7-hydroxymitragynine (7-OH).
See the following graphs from the CDC study.
Hospitalizations for single substance kratom reports increased from 43 in 2015 to 538 in 2025, that is 1,200%. Hospitalizations for multiple substance kratom reports increased from 40 in 2015 to 549 in 2025, 1,300%. Hospitalizations were higher among persons who were using multiple substances than single substance, kratom only users. A similar pattern was evident for serious outcomes, which are delineated in the following graphs.
There were 233 kratom associated deaths during 2015-2025; 184 (79%) involved multiple substances. “Opioids were reported in 62% of fatalities, followed by benzodiazepines (20%), stimulants (20%), and ethanol (19%).”
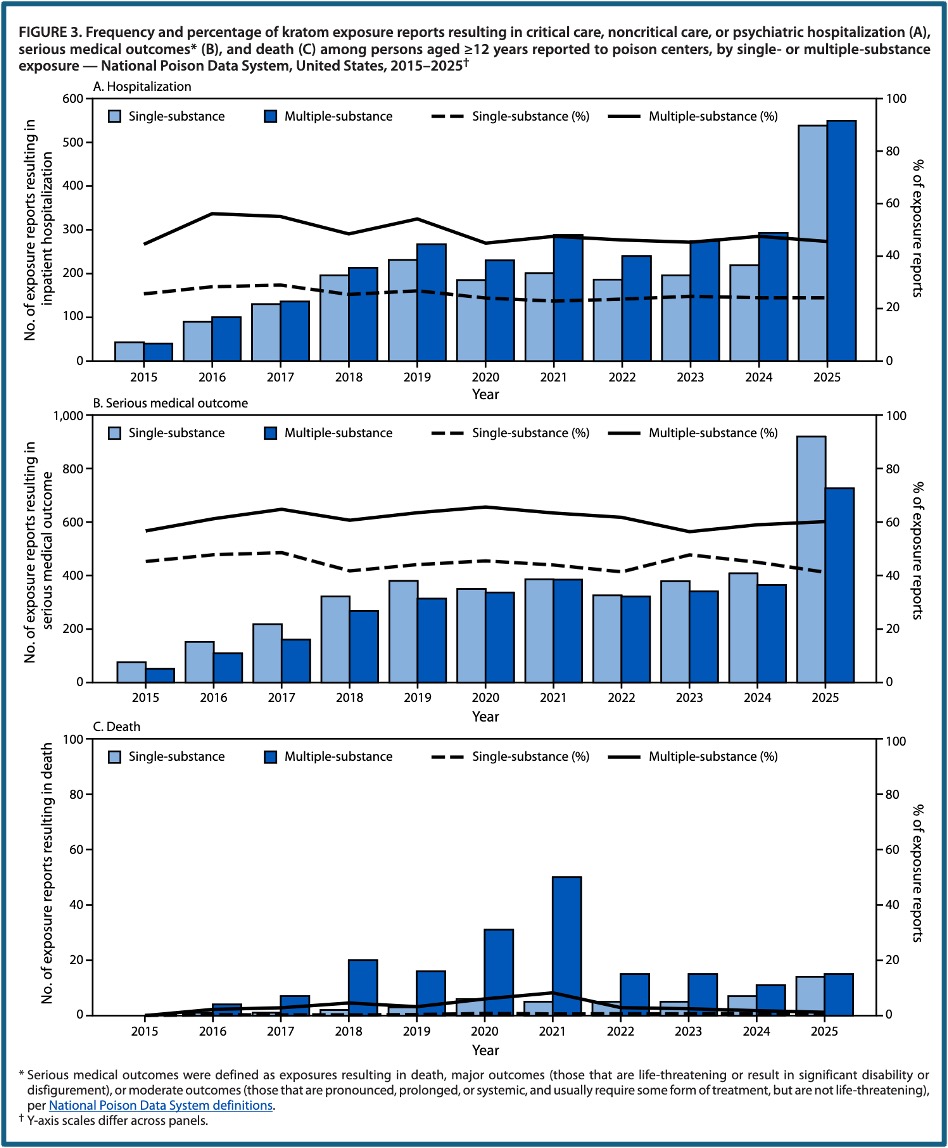
Together, these findings indicate that kratom use is increasing and expanding across demographic groups, underscoring a growing public health concern. In 2025, among all multiple-substance exposure reports, 60% resulted in serious medical outcomes and approximately one half required hospitalization. Enhanced surveillance and public health education could be beneficial given kratom’s widespread availability, lack of regulation, minimal medical oversight, and involvement in high-risk multi-substance exposures.
The findings in this report describe the impact of the rapidly evolving kratom market and highlight the important role poison centers can play as an early warning surveillance system to detect new trends and guide community partners, including clinicians, members of the public, and public health leadership. Severe outcomes were observed among persons who used kratom with other substances: approximately one half required inpatient hospitalization, and 79% of reported kratom-associated deaths involved multiple substances. Kratom use with alcohol, opioids, benzodiazepines, stimulants, and antidepressants might increase risk through additive pharmacodynamic effects on central nervous system pathways and through pharmacokinetic interactions that increase systemic exposure to substances used with kratom. This concern is heightened by the emergence of semisynthetic kratom products that have higher affinity for the opioid receptor, given that the majority of deaths involved kratom use with opioids. Psychiatric comorbidity might also compound harm. Previous studies indicate that approximately one third of kratom users met criteria for another substance use disorder, and approximately two thirds reported using kratom to manage depression or anxiety. Consistent with these findings, suicide attempts accounted for approximately one fourth of multiple-substance exposure reports, compared with only 6% of single-substance exposure reports, and antidepressants were involved in 14% of multiple-substance exposure reports, underscoring a connection between kratom use and mental health crises.
The Paradox of Kratom and Why the FDA is Cracking Down
In “How Kratom Hijacks the Brain,” Dr. Sanil Rege, an Australian psychiatrist explored the neurobiology, history and dangers of kratom. He said kratom is marketed as a natural herbal remedy. At low doses, it acts like a stimulant. It’s also used as an alternative opioid. “Kratom can energize you like coffee at one dose, sedate you like morphine at another, and in some cases, trigger psychosis, seizures and even liver failure.” The FDA is now warning about kratom, referring to it as “not appropriate for use as a dietary supplement,” and “not lawfully marketed as a dietary supplement.”
Kratom is native to southeast Asia, Thailand, Malaysia, and Myanmar. There, it’s known as Thang, kakuam, ketum and Biak. Traditionally, it’s chewed, brewed as tea, or smoked. “Historically, it was used by rural workers to combat fatigue, increase productivity and manage pain.” In modern times, it’s sold as powders, capsules, and extracts; both online and in supplement shops.
There are 3 to 5 million users of kratom in the US. It’s used recreationally and for self-medication to treat chronic pain, anxiety, and opioid withdrawal. Kratom has over 40 compounds, with the important ones being mitragynine and 7-hydroxymitragynine (7-OH). Mitragynine constitutes approximately 66% of the total alkaloids in kratom. 7-hydroxymitragynine (7-OH) only constitutes up to 2% of the total alkaloids in kratom, but is more potent, with the equivalent of 13 times that of morphine at the mu opioid receptors. Kratom also has an unpredictable metabolism, where mitragynine converts to 7OH in the liver, which means its potency can vary depending on dose, product quality and individual metabolism.
Mitragynine and 7-OH are both partial agonists, not full agonists like morphine. They also interact with other receptors—adrenergic, serotonin, and dopamine. The result is a hybrid pharmacology that acts as a stimulant at low doses and like an opioid at higher doses. Unlike morphine, kratom alkaloids avoid the beta-arrestin pathway, which is known to drive respiratory depression and constipation. “That’s why kratom doesn’t always cause the classic opioid side effects, leading users to think it’s safer.”
At low doses, kratom increases alertness, talkativeness and mild euphoria, while boosting physical energy. At higher doses, it leads to sedation, pain relief, and a warm opioid-like calm. Side effects can include nausea, sweating, constipation, itching, dry mouth, drowsiness, and appetite suppression. In severe cases, individuals may experience agitation, hallucinations, even seizure. Liver injuries, coma and even death may occur.
A 2019 study in the journal Pharmacology, “Kratom Use and Toxicities in the United States,” said kratom “commonly caused agitation (18.6%), tachycardia (16.9%), drowsiness (13.6%), vomiting (11.2%), and confusion (8.1%).” Serious side effects such as “seizure (6.1%), withdrawal (6.1%), hallucinations (4.8%), respiratory depression (2.8%), coma (2.3%), and cardiac or respiratory arrest (0.6%) were also reported.” The researchers concluded kratom was associated with significant toxicities and should not be considered to be safe. They thought it was a public health threat because it was available as an herbal supplement.
The long-term and dependency risks with kratom report kratom has a withdrawal effect of its own. “Users report tolerance, requiring escalating doses for the same effect. They report withdrawal, irritability, anxiety, insomnia, [and] muscle aches. Some describe it as milder than opioids, but harder to shake than caffeine.” There can be liver injury, kidney injury, thyroid dysfunction and lung injury.
There is a cognitive impact in long-term users—memory impairment and concentration difficulties. There are case reports of persistent psychosis. Now here is where it gets even darker, because the real danger isn’t always the kratom itself, but what’s hiding inside the product being sold. When you buy kratom powder, do you know what’s really in it? Kratom is legal in many places, but unregulated. Potency varies massively. Mitragynine’s content is inconsistent. Some products are spiked with synthetic opioids, which can lead to fatal overdoses.
Then in July of 2025, the FDA announced it was taking steps to restrict 7-OH products. The news release said “7-OH is an opioid that can be more potent than morphine. We need regulation and public education to prevent another wave of the opioid epidemic.” The availability of 7-OH online, in gas stations, corner stores and vape shops is a major concern because these products are sometimes disguised or marketed as kratom. The FDA recommended scheduling 7-OH products under the Controlled Substances Act.
Dr. Rege noted the FDA’s focus is not on the natural leaf, but on concentrated extracts because of the high binding affinity at opioid receptors, which has significant abuse potential. Natural kratom leaves may remain legal, but extracts, adulterated products and 7-OH concentrates could become illegal.
Kratom is both a problem and a potential solution for the opioid epidemic. Traditional users in Southeast Asia have a low incidence of severe harm. In the US and Europe, there are more problems because of high-potency extracts and adulterated products. “Scientists are studying mitragynine as a blueprint for safer opioid products because it avoids the beta-arrestin pathway.” So, kratom could inspire future treatments for pain, but in its current unregulated status, it risks becoming another phase of the opioid crisis.
I’ve been monitoring kratom and its unregulated status in this blog since 2015. See this link for past articles referring to kratom. I think I agree with Dr. Rege, that it is a problem and potential solution for the opioid epidemic. But the scientific research needs to be done to see if mitragynine can be developed into a safer opioid product. And the extracts, adulterated products and 7-OH concentrates need to become Schedule I Controlled Substances.



