
As medical marijuana began to be sold in Pennsylvania I speculated that a prediction by a co-sponsor of Senate Bill 3, that dry leaf marijuana would be sold in PA dispensaries sometime in 2018, was more bluster than reality. But it seems I was wrong. On April 16th, 2018 Governor Wolf announced that he supported changes to the existing state medical marijuana program that would allow dispensaries to sell dry leaf marijuana. Regulations to enact the recommendations will be available in the Pennsylvania Bulletin on May 12. Were the state legislators who voted for Senate Bill 3 aware a provision in it would permit an advisory board to approve the sale of dry leaf marijuana at a later date, even though the initial bill did not permit it? And were they aware there would be a move to sell dry leaf in dispensaries so quickly? Would they have voted for the Bill if they knew that was the goal?
Rachael Levine, the PA Health Secretary, announced on April 16th that she approved recommendations from the state’s medical marijuana advisory board to permit the sale of dry leaf “for patients with a qualifying medical condition.” The rationale to permit access to dry leaf marijuana was said to offer a lower-cost option to the concentrate forms. Allegedly the flower form is believed to be more effective in treating some medical conditions with better dosage control than the concentrate form ( a statement made without any supporting evidence). PA law still prohibits smoking medical marijuana or using it in edible form, but plant matter can be legally vaporized, meaning it can be heated, but not burned.
It’s not clear how that rule would be enforced once the marijuana is purchased and taken home. Dr. Levine said patients would be urged to follow the prescribed methods for administering the medical marijuana. “We are not looking for an intoxicating effect. We are looking for a medical effect.”
The Cannabist wrote about the proposed changes to allow the sale of dry leaf or flower marijuana in Pennsylvania. A cannabis consumer advocate said no state law would prevent certified medical marijuana users from buying the dry leaf product and smoking it legally, instead of vaporizing it. “I’m sure patients are going to go home and smoke it, and there’s nothing wrong with it. . . . This is how humans have used cannabis for 10,000 years and it’s how people should have access to it in Pennsylvania.”
In all, there were 21 proposed changes to Pennsylvania’s medical marijuana program. Additional changes included allowing physicians participating in the program to choose to not have their name listed in the public registry to encourage more physicians to participate. The number of qualifying medical conditions is to increase from 17 to 21. One of those additional medical conditions was “the use of medical marijuana as a substitute for treating opioid addiction.” This change barely passed, with six of the 12 voting advisory board members voting in favor and at least one person abstaining (More on this issue later). Another proposed change that would limit a practitioner’s ability to specify the form and dose of medical marijuana a patient should get was not approved. Governor Wolf’s statement said:
My administration is committed to ensuring patients who need and would benefit from this medicine have access to it. The final report of the Medical Marijuana Advisory Board continues to put patients first and will improve the program to give greater access to patients by breaking down financial and administrative barriers. Allowing dry leaf for vaporization will shorten the time it takes to get medication to dispensaries, expand options for the growing number of patients, and hopefully make the program less cost-prohibitive for some patients.
But is this just political rhetoric? Are Pennsylvania’s elected officials being maneuvered into a path toward the eventual legalization of recreational marijuana?
State Senator Daylin Leach predicted at the World Medical Cannabis Conference & Expo, held in Pittsburgh on April 21 and 22 of 2017, that medical marijuana in plant form would be available in dispensaries sometime in 2018. During a panel discussion at the Expo held at the David L. Lawrence Convention Center, he noted State Bill 3 had a section permitting the advisory board to make recommendations by April 2018 about changing the permitted forms of the drug. “But they will, because we’re appointing people to do that.” He believes that full legalization of recreational marijuana in Pennsylvania is inevitable.
State Senator Mike Folmer was another of the primary sponsors of State Bill 3. He said he’s not opposed to legalizing recreational marijuana, but he can’t “politically advocate” for it at this time. WESA said he recalled “how difficult it was to get enough Republicans on board with the medical marijuana program.” I wonder if those unnamed Republicans were aware that their approval of State Bill 3 had a loophole section permitting the advisory board to approve changes to the permitted forms of marijuana? Are they feeling manipulated into approving what was presented as a bill that would restrict the dispensing of dry leaf cannabis?
CBD vs. THC
Another issue with the approval of selling cannabis dry leaf in the dispensaries is making a clear distinction of the kinds of marijuana that will be sold. There seems to be very little effort made when discussing medical marijuana in Pennsylvania—either by the media or government officials—to distinguish cannabis with high levels of THC from strains with high levels of CBD. Tetrahydrocannabinol (THC) is psychoactive, while cannabidiol (CBD) is not. A helpful overview of the differences between THC and CBD can be found in: CBD vs. THC: Main Differences.
Both THC and CBD are present in mature cannabis flower. But different cannabis strains produce different amounts of the compounds. So what strains of cannabis will be sold for medical reasons in Pennsylvania and will they have high concentrations of THC or CBD? Will there be more high THC strains?
Cannabinoids like THC and CBD effect the endocannabinoid system (ECS), which is “named for the plant that inspired its discovery.” Until recently the ECS was an unknown part of the human body’s functions. It helps ensure the proper running of the body’s immune and central nervous system. Its discovery came about through the research efforts of Lisa Matusuda and her team at the National Institute of Mental Health (NIMH) in the early 1990s, where they first identified a THC-sensitive receptor in the brains of lab rats. “The endocannabinoid system is responsible for regulating balance in our body’s immune response, communication between cells, appetite and metabolism, memory, and more.” The cannabinoids in cannabis like THC and CBD interact with the ECS to produce their effects.
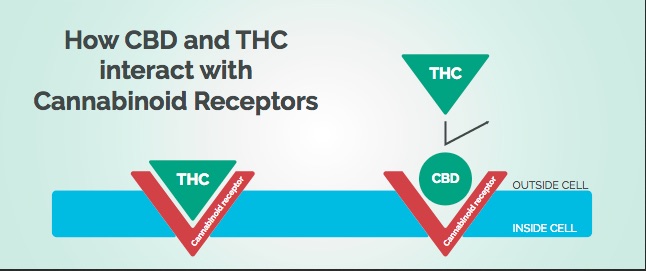
Another researcher team was able to identify two of the body’s naturally produced endocannabinoids, anandamide and 2-arachidonoyglycerol (2-AG). 2-AG is a full agonist of both CB1 and CB2 receptors. Anandamide is a partial agonist of both receptors and as a result, doesn’t trigger as powerful a physiological response. Cannabinoids like THC and CBD mimic the behavior of endocannabinoids like 2-AG and anandamide. THC activates CB1 receptors, producing the high effect. Although THC also activates CB2 receptors, there it is a partial agonist, meaning it does not have as strong of a physiological effect.
“CBD causes chemical changes by blocking receptors. It tends to have low affinity for both CB1 and CB2 receptors, and instead acts as an indirect antagonist of agonists.” In other words, CBD blocks other chemicals like THC from binding and activating the receptors, as shown in the following graphic in: CBD vs. THC: Main Differences:
 By modulating the endocannabinoid system, several diseases and conditions could possibly be treated, including: pain, inflammation, multiple sclerosis, anorexia, epilepsy, cancer, glaucoma, cancer, obesity, schizophrenia, cardiovascular disorders, Parkinson’s disease, Huntington’s disease, Alzheimer’s disease and Tourette’s syndrome.
By modulating the endocannabinoid system, several diseases and conditions could possibly be treated, including: pain, inflammation, multiple sclerosis, anorexia, epilepsy, cancer, glaucoma, cancer, obesity, schizophrenia, cardiovascular disorders, Parkinson’s disease, Huntington’s disease, Alzheimer’s disease and Tourette’s syndrome.
One of the main obstacles to the acceptance and use of cannabis as a medicine is its potential for psychoactivity from THC. BUT “this issue does not arise in a number of possible approaches to the regulation of the endocannabinoid system.” One way is when a non-psychoactive cannabinoid like CBD is used for therapeutic reasons. Another is when an antagonist to the CB1 receptor blocks THC from activating it. Are the cannabis strains and medical marijuana products being distributed in Pennsylvania formulated to minimize the euphoric activation of the CB1 receptor by THC?
Benefits of CBD
Josh Axe, a wellness physician, has listed “8 Proven Benefits of CBD.” On his list are 1) that CBD relieves pain and inflammation; 2) it has antipsychotic effects; 3) it reduces anxiety; 4) helps to fight cancer; 5) relieves nausea; 6) it may treat seizures and other neurological disorders; 7) it could lower the incidence of diabetes; and 8) it promotes cardiovascular health. Dr. Axe cited multiple references to support these claims. He acknowledged several health benefits with THC, including its antispasmodic, analgesic, anti-tremor, anti-inflammatory and appetite stimulating properties. However, there are multiple adverse effects from marijuana use that have been documented in studies primarily of recreational marijuana, which is high in THC. See “Marijuana Research Findings” for more information.
Approving “medical marijuana as a substitute for treating opioid addiction” is a broad and vague addition to the list of approved medical uses of marijuana in Pennsylvania. Does that mean an individual could use medical marijuana as a MAT (medication-assisted treatment) for an opioid misuse disorder? There is reliable evidence for marijuana (THC and CBD) to relieve pain, but that is different than treating opioid addiction.
According to the Chicago Tribune the Illinois Senate recently passed a bill that would allow patients to take an opioid prescription and a signed doctor’s note to a medical marijuana dispensary in order to substitute marijuana for pain relief. “The dispensary must verify approval from a doctor and ensure a patient is not already receiving medical marijuana through another means.” One of the bill’s sponsors said: the bill “keeps people from getting strung out and spiraling down.” The Chicago Tribune commented where that state Senator received at least $8,000 in campaign contributions from medical marijuana interests.
Opponents to the bill said lawmakers were helping medical marijuana dispensaries become profitable businesses by expanding the number of people who can use the drug. One lawmaker said: I just want to make note and remind people that the medical marijuana program was lobbied by people who now own it.” If support for the bill in Illinois was motivated by individuals looking to profit from it, that should be known. However, note again that it was directed to patients with an opioid prescription substituting medical marijuana for the prescription and not the vaguely defined use “as a substitute for treating opioid addiction.”
There was a report on the NPR program All Things Considered on April 2, noting: “Opioid Use Lower In States That Eased Marijuana Laws.” The article highlighted two studies published in JAMA Internal Medicine showing there was a decrease in Medicare and Medicaid prescriptions for opioids in states with liberal marijuana laws. One study found a 14% reduction in opioid prescriptions in states allowing easy access to medical marijuana. The finding was a correlation and thus doesn’t prove marijuana use would result in a reduction in the use of opioids. Nevertheless, “the findings suggest that expanding access to medical marijuana could help ease the opioid epidemic.” Again, this is not vaguely defined use as a substitute treatment for opioid addiction. One of the researchers said:
Like any drug in our FDA-approved pharmacopeia, it can be misused. There’s no question about it. So I hope nobody reading our study will say ‘Oh, great, the answer to the opiate problem is just put cannabis in everybody’s medicine chest and we are good to go.’ We are certainly not saying that.
The authors of the second study said while laws permitting marijuana use have the potential to reduce opioid prescribing in a population segment with a high risk for chronic pain use disorder and opioid overdose, “Nevertheless, marijuana liberalization alone cannot solve the opioid epidemic.”
Another study cited in the NPR report, “Cannabis Use and Risk of Prescription Opioid Use Disorder,” found cannabis use appeared “to increase rather than decrease the risk of developing nonmedical opioid use.” The lead author of the study said there was likely a role “for medical marijuana in reducing the use of prescribed opioids for the management of pain.” But it is a question of balancing risks and benefits, which is hard to do when the current studies are based on broad populations and not the at-risk populations as a whole. And once again, the potential is for individuals with pain issues to benefit from marijuana, not for it to be used as a substitute for treating opioid addiction.
Governor Wolf said he is committed to seeing that citizens of Pennsylvania who need medical marijuana get it. Secretary Levine said: “We are not looking for an intoxicating effect. We are looking for a medical effect.” Hopefully that means cannabis strains and medical marijuana products that are high in CBD and low in THC will be sold in Pennsylvania dispensaries while high THC products will be limited. It is also alarming that such a vague expansion of the permitted treatments, namely to use “medical marijuana as a substitute for treating opioid addiction,” could be included in the revised regulations. Let’s hope the government officials and regulators work to keep marijuana medical in Pennsylvania. But it is also apparent that there are others, perhaps including some of the sponsors of Senate Bill 3, who see the state’s approval of medical marijuana as a stepping stone towards recreational marijuana.
Documents detailing multiple revisions to Pennsylvania’s Medical Marijuana Program were posted online on May 12, 2018. They include permitting the sale of “dry leaf or plant form for administration by vaporization.” This can be smoked like recreational marijuana, although it is illegal in PA to do so. However, there is no clear way to enforce the restriction. As noted above, a pro cannabis activist acknowledged individuals would smoke, not vaporize the dry leaf product saying, “This is how humans have used cannabis for 10,000 years and it’s how people should have access to it in Pennsylvania.”
Also, opioid use disorder is now an approved medical condition to receive medical marijuana. The new regulation is vague and subjective. It seems to provide a loophole for individuals who have an opioid use disorder diagnosis to qualify for a medical marijuana card. The new regulation permitting medical marijuana for opioid use disorder reads: “Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions.” The documents describing the amended regulations are available here: http://cannabislawpa.com/updates-resour…/regulatory-updates/
Please share this information with others who may be concerned with the revised regulations so they can voice their concerns. Anyone troubled by these noted changes, or any others within the new guidelines can submit written comments, suggestions or objections regarding these amended temporary regulations to John J. Collins, Office of Medical Marijuana, Department of Health, Room 628, Health and Welfare Building, 625 Forster Street, Harrisburg, PA 17120, (717) 547-3047. The given email address for John Collins was invalid. I will update it here if I locate a valid one.



