JAMA Psychiatry recently published a study, “Incidence and Nature of Antidepressant Discontinuation Symptoms,” to examine the presence of antidepressant discontinuation symptoms and the incidence of discontinuation symptoms in individuals who stopped taking antidepressants. The review and meta-analysis indicated the mean number of discontinuation symptoms was below the threshold for clinically significant discontinuation syndrome and mood worsening was not associated with discontinuation. “Therefore, later presentation of depression is indicative of depression relapse.” However, upon closer examination, their results are more like a sleight-of-hand trick, or shutting the barn door after the horse has gone.
Mark Horowitz and Joanna Moncrieff wrote a response to the above study in The Conversation that was republished in ScienceAlert. They noted many of the academic authors of “Incidence and Nature of Antidepressant Discontinuation Symptoms” had close ties to drug manufacturers. They said the authors’ study “risks underestimating the potential harms to long-term antidepressant users by focusing on short-term, industry-funded studies.”
Horowitz and Moncrieff said there is growing recognition that stopping antidepressants, particularly with long-term use, can lead to severe and sometimes debilitating withdrawal symptoms. See “Antidepressant withdrawal effects and duration of use: a survey of patients enrolled in primary care psychotherapy services.” They said one of the main reasons it took so long to be recognized as a concern after the release of modern antidepressants was because withdrawal effects were said to be brief and mild.
This description was based on studies run by drug companies, where people had only taken the medication for eight to 12 weeks. As a result, when patients later showed up with severe, long-lasting symptoms, many doctors didn’t take them seriously because these experiences contradicted what the guidelines led them to expect.
Our recent research helps explain this mismatch. We found a clear link between how long someone takes antidepressants and how likely they are to experience withdrawal symptoms – and how severe these symptoms are. [See the following charts from their “Antidepressant withdrawal effects” study]
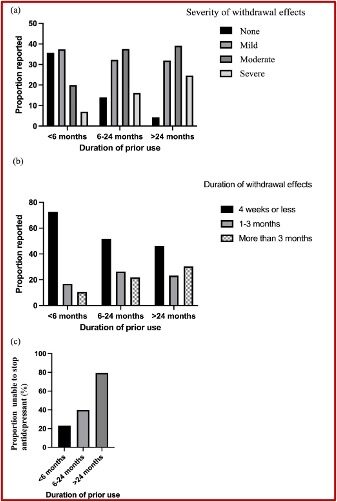
Patients who used antidepressants for less than six months had mild and brief withdrawal symptoms. “Three-quarters reported no or mild symptoms, most of which lasted less than four weeks.” However, one in four patients were unable to stop when they wanted to stop. Two-thirds of long-term users (more than two years) reported moderate or severe withdrawal effects; and 25% reported severe withdrawal effects. Almost one-third of long-term users had symptoms lasting more than three months; 80% of these patients could not stop taking their antidepressants despite trying.
There are around 2 million people on antidepressants in the England who have been taking them for over five years. In the US, there are at least 25 million people doing the same. “What happens to people in eight-to-12-week studies is a far cry from what happens to millions of people when they stop.”
History Repeating Itself
Horowitz and Moncrieff reasoned the review in the JAMA Psychiatry study looked like history repeating itself, as it reached the same conclusions as the initial research into potential antidepressant withdrawal. The researchers centered their analysis on studies with relatively short time periods of antidepressant use, with a likelihood of underestimating the risks of antidepressant withdrawal. The main analysis of the study was based on 11 trials comparing withdrawal symptoms in people who had stopped antidepressants with those who had continued them or stopped taking a placebo. Six of the trials were with people on antidepressants for 8 weeks, four for 12 weeks, and only one for 26 weeks.
They reported a slightly higher number of withdrawal symptoms in people who stopped their antidepressant, saying this did not constitute a “clinically significant” withdrawal syndrome. They then suggested the symptoms could be explained by the “nocebo effect,” meaning negative expectations cause people to feel worse.
In our view, the results are likely to greatly underestimate the risk of withdrawal for the millions of people on these drugs for years. The review found no relationship between the duration of use of antidepressants and withdrawal symptoms, but there were too few long-term studies to test this association properly.
The review probably underestimates, in our view, short-term withdrawal effects too by assuming that the fact that people experience withdrawal-like symptoms when stopping a placebo or continuing an antidepressant cancels out withdrawal effects from antidepressants. But this is not a valid assumption.
We know that antidepressant withdrawal effects overlap with side-effects and with everyday symptoms, but this does not mean they are the same thing. People stopping a placebo, report symptoms such as dizziness and headache, because these are common occurrences.
But symptoms following discontinuation of a placebo are typically milder than those experienced with antidepressants. “So deducting the rate of symptoms after stopping a placebo or continuing an antidepressant from antidepressant withdrawal symptoms is likely to underestimate the true extent of withdrawal.” The authors of “Incidence and Nature of Antidepressant Discontinuation Symptoms” suggested depression after stopping antidepressants is probably a return of depression, not withdrawal symptoms, because the rates of depression were similar to rates of depression in people who stopped taking placebo. “But this conclusion is based on limited and unreliable data (that is, relying on participants in studies to report such events without prompting, rather than assessing them systematically) from just five studies.”
Horowitz and Moncrieff concluded in their “Antidepressant withdrawal effects” study that withdrawal experiences were common. “The duration of prior use of antidepressants was identified as a risk factor for incidence, severity and duration of withdrawal symptoms, and ability to stop the medication.” There were few other characteristics independently associated with withdrawal outcomes. Brief users reported primarily mild and brief symptoms; and longer-term users reported mostly moderate to severe withdrawal effects. “Guidelines should be updated accordingly and patients informed of these risks when considering commencing, deciding on whether to continue and when stopping antidepressant treatment.”
For more information by Joann Moncrieff and Mark Horowitz on antidepressants, see: “Withdrawal or Relapse When Tapering with Antidepressants?,” “The Death of the Chemical Imbalance Theory?,” and “The Myth of the Serotonin Theory of Depression.”
Misdiagnosing Antidepressant Withdrawal
Mark Horowitz and James Davies authored an article for Psychiatry and Psychology, “Hidden Costs” that documented the clinical and research costs of mistaking antidepressant withdrawal for relapse. They observed that one of the commonest stories in psychiatric practice was a patient reporting their withdrawal symptoms after stopping an antidepressant was misdiagnosed as a relapse to a previous mental health condition, or the onset of a new mental or physical health condition. Misdiagnosis was explainable given the antidepressant mantra noted above, that from the beginning withdrawal effects were said to be “mild and brief.” Such guidelines were based primarily on industry studies lasting 8-12 weeks.
“However, even within these short-term trials not all patients experience brief and mild symptoms.” Pfizer researchers found that after just 8 weeks of venlafaxine (Effexor), 38.7% of patients were found to have moderately severe withdrawal symptoms, 3.2% severe symptoms, and 1.6% very severe symptoms. But as discussed above, most patients will avoid severe or protracted withdrawal symptoms after 8-12 weeks of antidepressant use.
Having said this, most patients take antidepressants for far longer than the 8–12 weeks covered by such trials – e.g., half in the UK and 70% in the USA have been taking them for over 2 years. As longer use is linked with more frequent and severe withdrawal effects, data from short-term studies can significantly mislead guidelines and practitioners. For example, a recent systematic review and meta-analysis by Henssler and colleagues significantly underestimated the incidence and severity of antidepressant withdrawal by relying mostly on data from such short-term industry trials (whilst also relying heavily on spontaneous reporting of withdrawal effects and retrospective analysis by clinicians – both known to under-estimate detection of withdrawal effects). Such research perpetuates the “brief and mild” withdrawal narrative in guidelines, by largely failing to detect the impact of long-term use, enabling the misdiagnosis of severe or prolonged withdrawal symptoms. Misdiagnosis is further reinforced by the lack of emphasis on withdrawal effects in diagnostic guides like the DSM and ICD.
This situation raises an important question: how many mental health diagnoses in clinical practice result from misdiagnosed withdrawal? Cosci and colleagues have taken on the important task of trying to answer this question.
In Psychotherapy and Psychosomatics, Cosci and colleagues examined 74 patients referred to their clinic for reduction, rationalization, and discontinuation of psychotropic medications. From that group they concentrated on those who had stopped antidepressants and assessed them for withdrawal symptoms. Horowitz and Davies said Cosci and colleagues found that if withdrawal effects were not taken into account, “58 patients would have had a current mental disorder misdiagnosed, 13 would have had a past disorder misdiagnosed and the remaining 3 would have had both current and past disorders misdiagnosed.” The most likely misdiagnoses were major depression and panic disorder. This was understandable, as low mood, suicidality, anxiety, insomnia, and panic are all common symptoms of antidepressant withdrawal; and they overlap with the diagnostic criteria for these disorders.
The authors recommend the use of an exclusion criterion for withdrawal effects to avoid misdiagnosis of relapse. “Implementing this would require using a withdrawal instrument like the DID-W1 or DAWSS, alongside the DSM, or updating the DSM to include such an exclusion criterion.”
Cosci’s findings have significant implications for clinical practice. Many patients exhibiting typical withdrawal symptoms are misdiagnosed due to reliance on inaccurate guidelines or diagnostic tools, leading to protracted withdrawal syndromes going unrecognised by health services. Consequently, such patients often feel abandoned by services, having instead to rely on themselves or on friends and family for care and support for harms that can be highly disabling (e.g., leading to job loss, relationship breakdown and even suicide).
Furthermore, systemic misdiagnosis means that the health system itself remains unaware of how much harm is being caused by withdrawal effects and how significant the cost to the healthcare system and wider economy. A recent analysis quantifying the considerable cost of unnecessary antidepressant prescriptions to the health system (millions of pounds), is likely to be dwarfed by the costs of emergency presentations and admissions caused by withdrawal and loss of productivity to the wider economy.
Horowitz and Davies concluded the Cosci and colleagues’ paper underlined the importance for clinicians and researchers to consider withdrawal effects when patients present with distressing symptoms after reducing or stopping antidepressants. “Ignoring this can lead to misdiagnosis, gaslighting, ongoing unnecessary treatment, exaggeration of the relapse prevention properties of these drugs, and a failure by health systems to acknowledge the harm caused by this class of drugs, including potential long-lasting brain injuries (or dysfunction).”
Reflecting on Horowitz’s and Moncrieff’s comment that the conclusions of “Incidence and Nature of Antidepressant Discontinuation Syndromes” looked like history repeating itself, I think a more accurate metaphor would be the conclusions look more like an attempt at a sleight-of-hand trick with the data on antidepressant “discontinuation” syndrome.



