When the largest pharmacy benefit company in the U.S. with revenues of $104 billion publishes a study of patients’ use pain medications, it gets some attention. That was exactly what happened when Express Scripts published “A Nation in Pain.” FiercePharma and The New York Times, among others, highlighted some disturbing trends with the prescribing habits of painkillers. Around 60% of the patients taking opiates were also prescribed other sedative drugs, like muscle relaxants and benzodiazepines—a great way to overdose and die.
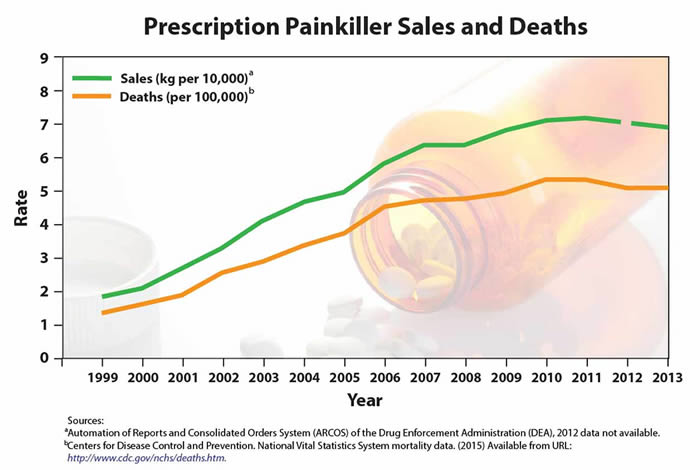
The CDC has said that the U.S. is in the midst of a prescription painkiller overdose epidemic. Since 1999, the amount of prescribed painkillers has almost quadrupled. But there hasn’t been an overall change in the amount of pain being reported. “Every day, 44 people in the U.S. die from overdose of prescription painkillers, and many more become addicted.” In 2013, that meant more than 16,000 deaths from painkillers. These overdoses often involved benzodiazepines. Almost 7,000 people are treated in ERs each day for their misuse of prescription painkillers. The most commonly identified drugs in overdose deaths include:
- Hydrocodone (e.g., Vicodin)
- Oxycodone (e.g., OxyContin)
- Oxymorphone (e.g., Opana)
- Methadone (especially when prescribed for pain)
“A Nation in Pain” looked at 6.8 million insured Americans of all ages who filled at least one prescription for an opioid to treat either short-term or long-term pain from 2009 through 2013. Short-term users were defined as patients who were prescribed an opiate pain medication for a total supply of 30 days or less within a one-year period. Long-term users were those prescribed an opiate pain medication for more than a 30-day supply in a one-year period. Some of the key findings of their study included a decline of 9.2% in the number of Americans filling a script for opioids between 2009 and 2013 (See the graphic below).
 But this decline was offset by an increase of 8.4% in the number of prescriptions filled and the number of medication days per prescription. The number of short-term users declined 11.1%, while the number of long-term users remained constant. Nearly half (46.9%) of long-term patients continued to use painkillers for three years or longer. “Almost 50% of those patients were taking only short-acting opioids, putting them at higher risk of addiction.” Of the nearly 60% of patients noted to be using potentially dangerous and fatal drugs in combination with their painkillers, 33% were using benzodiazepines. The most common cause of overdose deaths with multiple drugs involves opioids and benzodiazepines.
But this decline was offset by an increase of 8.4% in the number of prescriptions filled and the number of medication days per prescription. The number of short-term users declined 11.1%, while the number of long-term users remained constant. Nearly half (46.9%) of long-term patients continued to use painkillers for three years or longer. “Almost 50% of those patients were taking only short-acting opioids, putting them at higher risk of addiction.” Of the nearly 60% of patients noted to be using potentially dangerous and fatal drugs in combination with their painkillers, 33% were using benzodiazepines. The most common cause of overdose deaths with multiple drugs involves opioids and benzodiazepines.
A majority of patients (58.5%) were using opiate pain medications with other prescription drugs that carry safety risks when used concurrently. Among long-term opioid patients, 29.2% had prescriptions for benzodiazepines in the same month. Opioids, muscle relaxants and benzodiazepines all suppress the respiratory system. Taking them concurrently can increase these reactions exponentially.
While there could be rare instances when opioids and benzodiazepines or muscle relaxants may be appropriate to prescribe together, seeing these potentially dangerous mixtures used so commonly by such a high percentage of patients is of great concern.
Many patients were taking two or more short-acting opioids at the same time; 27.5% of the long-term opioid users were doing so. This combination of longer-term usage and concurrent usage of two or more short-acting opioids was a recipe for developing drug dependence and addiction. Of the patients taking these potentially dangerous combinations of medications, two-thirds (66.6%) were prescribed the drugs by two or more physicians. Almost 40% filled them at two or more pharmacies. Glen Stettin M.D., a Senior Vice President at Express Scripts said better coordination of care is needed to correct this problem.
People looking to abuse controlled substances will often attempt to obtain prescriptions from multiple prescribers; and fill prescriptions at multiple pharmacies. So Express Scripts has developed programs to counter the abuse by restricting certain patients to one pharmacy, and in some cases, to one prescriber. But drug addicts are nothing if not determined and ingenious. The following story may seem extreme, but with my experience working with addiction, I could see it happening.
Lynne Nowak, M.D., the Medical Director of Personal Health Solutions at Express Scripts told of a patient admitted to her hospice practice with a terminal illness. The patient was taking high doses of both short-acting and long-acting opioids, along with benzodiazepines and other medications. After gathering information and additional medical records, Doctor Nowak and her team discovered that the patient had fabricated a terminal illness and admitted himself to hospice care to get the medications.
In an appendix, Express Scripts indicated the top opioids in the U.S. according to their market share in 2013 were:
- •Vicodin®/hydrocodone with acetaminophen (46.1%);
- •Ultram®/Tramadol (14.7%);
- •Percocet®/oxycodone with acetaminophen (13.6%);
- •OxyContin®/oxycodone (8.3%);
- •Tylenol® with Codeine/codeine with acetaminophen (3.8%).
The huge preference for Vicodin® will likely fade by 2015, as it was reclassified upwards as a Schedule II controlled substance in October of 2014. This means that there will be greater restrictions on refills. Schedule II prescriptions require a physical prescription (no pharmacy call-ins) and a face-to-face visit with the prescriber. Ultram®/Tramadol is a Schedule IV controlled substance, and I expect that we will see an increase in how often it is prescribed with the increased restrictions on Vicodin®.