
Apparently, there are at least three different “amateur nights”: the night before Thanksgiving, which is also known as Blackout Wednesday or Drinksgiving, New Year’s Eve, and St. Patrick’s Day. What these so-called “amateur” nights have in common are they are times when people drink more than they are used to, and often experience negative consequences as a result. And as implied, the majority of the drinking is done by individuals who normally don’t drink to excess. There is also a term for this kind of behavior—binge drinking.
The NIAAA, the National Institute on Alcohol Abuse and Alcoholism, defined binge drinking as a pattern of drinking that brings blood alcohol concentration (BAC) to .08 or higher. This corresponds to 5 or more drinks for men or 4 or more for women in 2 hours. The National Survey on Drug Use and Health (NSDUH), conducted by SAMHSA, the Substance Abuse and Mental Health Services Administration, defined binge drinking as 5 or more alcoholic drinks for males or 4 or more alcoholic drinks for females on the same occasion.

The CDC and the NIAAA both define heavy drinking similarly: men who consume five or more on any day or 15 or more per week; and women who consume 4 or more on any day or 8 or more per week. The CDC also created a catchall term—excessive drinking—that includes binge and heavy drinking, as well as any alcohol use by people younger than 21 and drinking while pregnant. Excessive alcohol use caused 178,000 deaths in 2020-2021, which was a 29% increase since 2016-2017. This results in 488 deaths each day, about 20 people every hour. HealthDay said 1 in 6 adults in the U.S. are binge drinkers; and 25% of them binge on a weekly basis. “Binge drinking accounts for most cases of excessive alcohol use, and it’s distinct from alcoholism and alcohol use disorder (AUD).”
Binge drinking and alcohol use disorder are two different things. According to Dr. Lawrence Weinstein, the difference between binge drinking and meeting the clinical diagnostic criteria for an alcohol use disorder is based on the element of control. “Alcohol addiction is partially defined as the inability to cease consumption despite the negative consequences of alcohol intake, the need to consume more to reach the desired effect, and intense cravings.” A binge drinker doesn’t experience those symptoms.
Policy Genius, a website with guides for auto, home and life insurance, gave the following drunk driving statistics for 2024. From 2018 to 2022, there were 3,722 fatal car crashes during the holidays with a drunk driver. That is approximately 37.4% of all fatal car accidents occurring during the holidays (10,083). And this is higher than the percentage of fatal crashes involving a drunk driver during non-holiday times (29.4%). See the following table, taken from the Policy Genius link for drunk driving statistics.
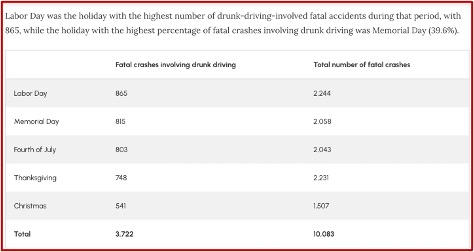
Note where the three so-called “amateur” nights aren’t included in their holiday statistics. Labor Day had the highest number of drunk-driving fatalities, with Memorial Day being the holiday with the highest percentage of fatal crashes involving drunk driving (39.6%). In 2024, there were 4,214 deaths involving a drunk driver during the holidays, 38% of all car accident fatalities during the holidays. Overall, I think we can say that in addition to the three amateur nights, the holidays noted above are also times to avoid binge drinking and driving.
The Pennsylvania State police reported they responded to more fatal wrecks and made more DUI arrests over the 2024 Thanksgiving weekend compared to 2023. Troopers investigated 1,075 vehicle crashes statewide; 64 were alcohol related. Seven deaths occurred and there were 552 DUI arrests.
Unfortunately, car accidents aren’t the only adverse health affect that can occur with binge drinking. HealthDay noted other health risks include: falls, burns, drowning. There can be acts of violence including suicide, homicide, sexual assault and partner violence. Not only is there a risk of sexual assault, risky sexual behaviors can lead to unintended pregnancies or sexually transmitted diseases, including HIV. And remember, even if you and the party in your car carefully avoided binge drinking, or have a designated abstinent driver, others on the roads for holidays and amateur nights may not take the same precautions.
Curbing Binge Drinking?
So, what are your options if the statistics described above have you concerned with the higher risks of drinking and driving on holidays and so-called amateur nights? The New York Times reported on a study that suggested, “Binge Drinking May Be Curbed with a Pill.” The article commented that binge-drinking may be seen as a harmless way to celebrate, party or relax, since there is such a low percentage of this type of drinker becoming dependent upon alcohol. “But it is considered a major risk factor for alcohol-related illness and injuries, and it heightens the possibility that an individual will develop an alcohol disorder.”
The study by Glenn-Milo Santos et al, published in the American Journal of Psychiatry, sought to “determine the efficacy of targeted naltrexone” in men who binge drink and have mild to moderate alcohol use disorder. The results of their study found that those who took naltrexone at least 2.5 days per week not only reduced any binge drinking, but also the number of binge-drinking days. “Moreover, the study showed sustained reductions in alcohol use patterns 6 months after treatment, suggesting that targeted naltrexone can result in lasting benefits for this population.” The study population was limited to sexual and gender minority men (SGM), but the results would likely apply to all males regardless of their sexual or gender identity.
In summary, we found that targeted use of oral naltrexone was efficacious in reducing alcohol use and craving among SGM who binge drink and have mild to moderate AUD, with sustained effects 6 months after treatment. Retention and treatment engagement were also high. Taken together, these data support the use of targeted dosing of oral naltrexone to address binge drinking in SGM with mild to moderate AUD.
The NYT article said this practice is more widely embraced in Europe, where the medication nalmefene was approved in 2013 for similarly targeted dosing. A physician-scientist with the NIH, Dr Leggio, said this study was “very important” because most people, like the study’s participants, have milder alcohol use disorders. The lead author for the study said: “Increasing awareness that there are effective medicines that can help people with their alcohol use is important in and of itself.”
The study’s approach applies a technique called the Sinclair Method, which is the subject of a book by Roy Eskapa, The Cure for Alcoholism. According to Eskapa, the book’s title means what it says: “Addiction to alcohol can now be cured—not through abstinence, but by always taking a medication [nalmefene or naltrexone] an hour before drinking alcohol.” The reduction in cravings is progressive, with the strongest effects in evidence three to four months after beginning to use the Sinclair Method. “The benefits continue increasing indefinitely so long as you take naltrexone [or nalmefene] if and when you drink.” The basic premise of the treatment method is that addiction is a learned behavior that has become so entrenched that the addict can no longer control it.
Like Eskpa, the Glenn-Milo Santos et al study and the NYT article found that after 12 weeks, those given naltrexone reported binging less frequently and consuming less alcohol than those given a placebo. Naltrexone blocks endorphins and reduces the euphoria of alcohol intoxication. Similarly, the Sinclair Method discussed how it “removes the neural changes that have developed in the brain, causing alcohol craving and excessive drinking.” The difference is the Glenn-Milo Santos et al study applies the Sinclair Method to binge drinking and those who have mild or medium alcohol use disorder.
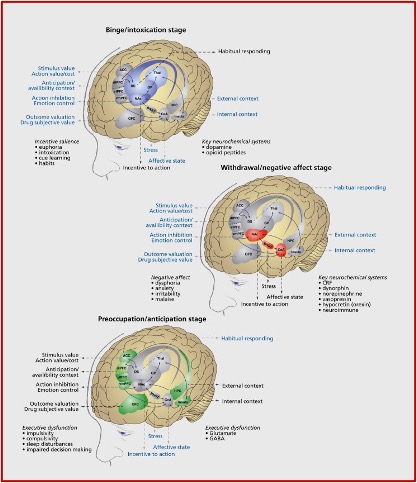
George Koob, the director of the NIAAA, theorizes that substance use disorder progresses through three stages: binge/intoxication, withdrawal/negative effect and preoccupation/anticipation. These stages are said to represent diverse neurobiological mechanisms involved in the transition from recreational to compulsive drug use, from positive to negative reinforcement. Progressing from recreational to compulsive substance use is associated with “downregulation of the brain reward systems and upregulation of the brain stress systems.”
Individual differences in the neurobiological systems that underlie the processing of reward, incentive salience, habits, stress, pain, and executive function may explain (i) the vulnerability to substance-use disorder; (ii) the diversity of emotional, motivational, and cognitive profiles of individuals with substance-use disorders; and (iii) heterogeneous responses to cognitive and pharmacological treatments. Characterization of the neuropsychological mechanisms that underlie individual differences in addiction-like behaviors is the key to understanding the mechanisms of addiction and development of personalized pharmacotherapy.
See the following figure illustrating the three stages of the addiction cycle found in the above-linked article. Remember that current DSM-5 language on substance use disorders (SUD) has three levels, mild, moderate and severe. The NYT and NIH officials have suggested that the categories mild to moderate SUD be understood as “preaddiction.” Earlier editions of the DSM distinguished between substance abuse and dependence or addiction.
 The rebranding of the earlier stages as preaddiction was recommended as a way to underscore the need for early intervention, similar to what the diabetes field did by identifying and treating prediabetes. Dr Leggio said: “If we attack the medical problem right away and early on, you cannot only treat the problem but prevent the development of the more severe forms of the disease.” Intervening into the progressive transition from recreational to compulsive drug use is a good thing, but there are some potential issues with trying to curb your binge drinking with naltrexone or nalmefene.
The rebranding of the earlier stages as preaddiction was recommended as a way to underscore the need for early intervention, similar to what the diabetes field did by identifying and treating prediabetes. Dr Leggio said: “If we attack the medical problem right away and early on, you cannot only treat the problem but prevent the development of the more severe forms of the disease.” Intervening into the progressive transition from recreational to compulsive drug use is a good thing, but there are some potential issues with trying to curb your binge drinking with naltrexone or nalmefene.
Naltrexone may reduce the quantity and frequency of alcohol consumption by interrupting or negating the euphoric response from drinking, but it does not necessarily impact the effect of alcohol on other areas of the brain like the prefrontal cortext, the part of the brain influencing judgment and self-control; or your blood alcohol level. There is a potential, then, that you would not feel that you were drunk, but blood work or a breathalyzer would indicate you to be at or above the .08 BAC level. And this is enough to negatively effect your driving judgement; or your self-control over doing the dangerous or stupid things people do when they have been binge drinking; or result in an arrest for DUI. Don’t think that naltrexone can lower your risk of negative consequences from binge drinking on the next holiday or amateur night.
For more information on the Sinclair Method, curing drunkenness, or the reward pathway of the brain and addiction, see; “Dimming the Experience of Pleasure and Addiction,” “A ‘Cure’ for Alcoholism,” or “Sure Cure for Drunkenness.”



