
On July 15, 2025, the FDA sent out seven warning letters to companies for illegally marketing products containing 7-hydroxymitagynine, also known as 7-OH, a partial agonist at the µ-opioid receptor found in kratom. The FDA has a growing concern about opioid products being marketed and sold online and in smoke shops, gas stations, and corner stores. “While 7-OH occurs naturally in trace amounts in kratom, the Agency’s letters focus on concentrated 7-OH products such as tablets, gummies, drink mixes, and shots, which may be dangerous.”
7-OH is not lawful in dietary supplements and cannot be lawfully added to conventional foods. Additionally, there are no FDA-approved drugs containing 7-OH, and it is illegal to market any drugs containing 7-OH. Consumers who use 7-OH products are exposing themselves to products that have not been proven safe or effective for any use.
The warning letters address the illegal marketing of products that contain 7-OH. Some of these products are adulterated foods, others are dietary supplements with enhanced levels of 7-OH that don’t meet the relevant safety standard. Others are presented as unapproved new “drugs” with unverified claims to relieve pain and manage anxiety. Once again, “There are no FDA-approved drugs containing 7-OH, and it is illegal to market any drugs containing 7-OH.”
Availability of Kratom and Sometimes Death
The global kratom market was valued at $2.19 billion in 2024 by MMR (Maximize Market Research) and is expected to grow to $7.80 billion by 2032. The North American kratom market is expected to expand at an increasing rate between 2025 and 2032. There was a 600% increased demand for kratom for medical purposes over the past five years. In 2020, the American Kratom Association estimated 10-16 million people in the US used kratom in some form. Current estimates of kratom users vary from just under 2 million to the American Kratom’s estimate.
The North American Kratom Market held the major share of the global market and is expected to grow during the forecast period due to in part to the opioid crisis. This led people to seek out safer alternatives to prescription opioids. Currently, an estimated 5.5 million people in the US use kratom. In the country, kratom is mainly available for purchase online and in head shops, gas stations, vaping establishments and corner stores. It is inexpensive, selling for nine to twenty dollars per ounce on the Internet.
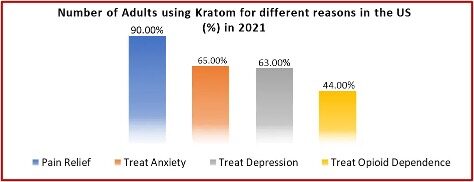
There are four primary reasons adults in the US gave in 2021 for using kratom: pain relief, anxiety, depression, and to treat opioid dependence. Many individuals are changing to kratom as an alternative to prescription painkillers, seeking natural pain relief, or for assistance with opioid withdrawal. Six states have made kratom illegal to use. Others have established age restrictions for kratom products. The largest percentage of kratom users report using it for pain relief. See the following graphic taken from the linked article on the global kratom market.
The Washington Post wrote in “They take kratom to ease pain or anxiety. Sometimes, death follows” that kratom was listed as “contributing to or causing at least 4,100 deaths in 44 states and D.C. between 2020 and 2022.” A considerable majority of those deaths involved other drugs in addition to kratom. Dozens of wrongful death lawsuits involving kratom have been filed nationally.
The CDC’s latest analysis, drawn from state overdose fatality records and completed at the request of The Post, found that kratom was implicated — at least in part — in 846 fatal overdose cases in 30 states and D.C. in 2022, the last full year for which data is available. That was up from 834 in 2021 and 663 in 2020. Most cases involved other substances. Kratom was listed as the sole substance causing death in 56 people in 2022, 68 in 2021 and 58 in 2020. The CDC analysis did not include several populous states.
In Texas, the number of deaths between 2020 and 2022 was 224. In Michigan, the total for that three-year span was 253 fatal cases, all in conjunction with other drugs such as opioids. In California, according to a health department analysis completed at The Post’s request, kratom was implicated in 242 deaths in those three years, with 27 blamed solely on the herb. In Florida, state statistics show, kratom was a factor in 525 deaths during that period.
Researchers say kratom seems to enhance the effects of certain prescription medications by interfering with the enzymes that break them down. “Researchers at Washington State University are launching a clinical trial to explore how kratom-infused tea affects the processing of the painkiller oxycodone.” Experts say it’s hard to separate the effects of kratom when it’s mixed with other drugs. A toxicologist said: “I think a lot of these kratom deaths are really due to misuse, not so much abuse. . . You take enough kratom, you can put yourself in harm’s way and die.”
A November 2024 study published in the American Journal of Public Health, found that kratom was available at 72% of tobacco specialty stores. The lead researcher said even in states where it was banned, many stores still sold it. This widespread availability leads to greater risks of addiction. See “Despite Federal Warnings, Kratom Still Readily Available Across US” for a by-state graphic representation of kratom’s availability.
Kratom’s Emergence as an Addictive Substance
Medscape Medical News said interest in kratom has dramatically increased in the U.S. over the past ten years. The recent surge in use and availability of products with 7-OH has some experts worried about the addictive properties of 7-OH. “Since late 2023, there has been a surge in “kratom” products marketed as ‘7-OH,’ ‘7-Hydro,’ or ‘legal morphine.’” Even the American Kratom Association (AKA) issued a consumer alert earlier this year about synthetically concentrated 7-OH products, advising they are being marketed as “kratom.”
The AKA’s “Consumer Alert on 7-OH Products” warned that 7-OH products were being deceptively labeled and markets as “kratom” products. “This false labeling deliberately misleads and confuses consumers who seek traditional kratom product formulations.” The AKA said current scientific research differentiates between mitragynine-dominant products [MG], which are traditionally recognized as kratom, and those containing synthetically concentrated levels of 7-OH. “Kratom, a botanical substance known for its mitragynine content, should not have 7-OH exceed 2% of the overall alkaloid content in any product marketed and labeled to be kratom.”
The most well-studied compounds in kratom are mitragynine, making up about 60%-65% of dried leaves, and 7-OH, which is only evident in trace amounts—often less than 0.05% of the leaf. At low doses, mitragynine yields mild stimulant and mood-boosting effects. But concentrated 7-OH preparations are 30-40 times more potent at opioid receptors “and produce rapid-onset analgesia, euphoria, respiratory depression and classic opioid-type withdrawal.”
A 2018 Medscape article, “’No Doubt’ Kratom Is an Opioid with High Abuse Potential,” did a series of experiments with rats and found that MG did not have abuse or addiction potential, while 7-HMG (a former term for 7-OH) did and could lead to an increased use of other opiates. Apparently at that time, there weren’t any 7-HMG/7-OH products on the market. “No one has sold 7-HMG on its own, but it’s possible that that could happen, and so it’s important to know that there is a possibility of abuse of that particular compound.”
MMR said kratom effects are dose dependent. At higher doses (5 to 15 g), it has sedative opioid-like effects, but at lower doses (1 to 5 g), it has cocaine-like stimulant effects. At higher doses, a pattern of symptoms occurring with opioids occurs: profuse sweating, dizziness, and nausea, which give way to euphoria. However, even traditional kratom has been noted to result in tolerance and addiction. “There are adverse effects associated both with acute overdose/toxicity and with chronic use. Chronic users also suffer tremors, frequent urination, anorexia, weight loss, seizures or psychosis. They suffer from withdrawal symptoms ranging from aggression to insomnia.”
Frontiers in Pharmacology published an updated, comprehensive review of the abuse potential of kratom, “Kratom Abuse Potential 2021: An Updated Eight Factor Analysis.” The researchers concluded there was no imminent public health threat or a high degree of pharmacological abuse potential that would justify scheduling kratom as a controlled substance. These findings were consistent with US survey data indicating relatively low self-reported kratom addiction rates. Most people described their MG use “to manage pain, depression, anxiety, opioid and other drug use disorders and withdrawal, and to increase alertness, focus and work performance.” Additionally, kratom dependence and withdrawal was typically weaker and more readily managed relative to opioids. The researchers concluded:
Further analysis and public input regarding kratom and its chemical components are needed before any scheduling should be undertaken. It is important that we have additional information to justify scheduling such as:
- A scientific assessment of how many Americans utilize kratom, and an understanding of the geographic and demographic distribution of these users (Factors 4, 5);
- A scientific assessment of the actual scale and degree of dependence and/or addiction of Americans utilizing kratom (Factors 1, 5, 7);
- A scientific determination based on data whether kratom actually serves as a gateway drug that promotes further use of more dangerous opioids (Factors 1, 4, 5).
- A valid prediction of how many kratom users will suffer adverse consequences if kratom is no longer available, including among people with intractable pain, psychological distress, risk for suicide; and/or people who might transition to proven deadly opioids such as prescription opioids, heroin, or fentanyl.
- A scientifically valid assessment of causality in the current few deaths in which kratom was co-utilized with known lethal drugs such as fentanyl (Factors 1, 2, 3, 5 and 6).
The article in Frontiers in Pharmacology seems to focus its attention and recommendations on what the AKA described as MG—traditional kratom—and not 7-OH. And it would seem the article can also mislead and confuse consumers seeking traditional kratom products. As the AKA said in their “Consumer Alert on 7-OH Products,” the AKA relies on scientific research that clearly differentiates between mitragynine-dominant products and those with synthetically concentrated levels of 7-OH that are marketed as kratom. “Kratom, a botanical substance known for its mitragynine content, should not have 7-OH exceed 2% of the overall alkaloid content in any product marketed and labeled to be kratom.” Any product with over the 2% of overall alkaloid content is not kratom and consumers should avoid them.
In addition, the AKA will (1) report any violative 7-OH products marketed and mislabeled as being a traditional kratom product to the Federal Trade Commission; and (2) any kratom or 7-OH products that make health claims not permitted under the Dietary Supplement Health and Education Act (DSHEA) to the Food and Drug Administration.
The AKA will publish and maintain an updated list of 7-OH products for consumer review that the AKA believes are improperly being marketed as kratom products and that will be referred to the Federal Trade Commission for their review and appropriate enforcement action for deceptive marketing. See the American Kratom Releases page for ongoing list.
Reining in the unregulated problems with 7-OH is the responsible thing to do with these so-called kratom “products” and it seems the AKA is heading in the that direction with its recommendations. Unregulated kratom is a problem.



