Misdiagnosing Substance Use

© adiruch | 123rf.com
Allen Frances doesn’t like the DSM-5 and you can hear him say so here. He said our mental health system was in a mess. And he is afraid that with DSM-5, it will get even worse. “People who are essentially normal are being diagnosed with mental disorders they don’t have.” Small changes in the diagnostic system can result in tens of millions of normal people qualifying for a diagnosis. He used himself as an example, stating how he would qualify for several of the DSM-5 disorders. Typical symptoms of grief over his wife’s death, lasting beyond two weeks, would have signified him as having a Major Depressive Disorder.
Anther mistake was combining what had been two different diagnoses of substance use in the DSM-IV—Substance Abuse and Substance Dependence—into one: Substance Use Disorder. Substance Abuse was when someone had recurrent, but intermittent, trouble from recreational binges. Substance Dependence was a continuous and compulsive pattern of use, often with tolerance and withdrawal. The majority of substance abusers “never become addicted in any meaningful sense.”
The two DSM IV diagnoses have radically different implications for treatment planning and for prognosis. Artificially lumping them together in DSM-5 forces inaccurate diagnosis, loses critical clinical information, and stigmatizes as addicts, people whose substance problem is often temporary and influenced by contextual and developmental factors.
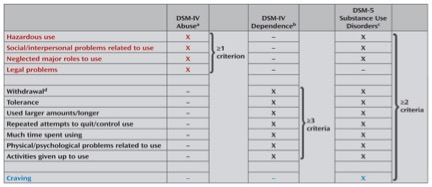
Hasin et al., “DSM-5 Criteria for Substance Use Disorders: Recommendations and Rationale,” presents the rationale used by the DSM-5 workgroup for substance use disorders for its changes, particularly combining abuse and dependence into one disorder. They recommended the combination as well as dropping one diagnostic criteria (legal problems) and adding one (craving). Two criteria are required to diagnose a Substance Use Disorder. The number of criteria met will indicate mild (2 to 3 criteria), moderate (4 to 5), and severe disorders (6 or more). The following chart, taken from the article, illustrates the changes from DSM-IV to DSM-5.
Frances is not alone in seeing value with two distinct types of substance use disorder. Carleton Erickson in The Science of Addiction noted how the distinction allowed for the differentiation between individuals with drug-related problems who could stop using when they wished (substance abusers), and others who had the disease of chemical dependence. Chemically dependent people have a dysregulation of the mesolimbic dopamine system and generally cannot stop using drugs without intensive intervention into their drug use problems. “According to these criteria, drug abuse in intentional, ‘conscious,’ or voluntary. Drug dependence is pathological and unintended.”
In his article, “DSM-5 Made a Mistake Eliminating Substance Abuse,” Allen Frances indicated the DSM-5 workgroup for substance use disorders based its rationale for dropping Substance Abuse on studies suggesting the distinction was hard to make. He said the results of the studies were not definitive. Moreover, their interpretation was flawed by what he said was a basic DSM-5 misunderstanding of the nature of psychiatric diagnosis. “All DSM disorder overlap with other DSM disorders and also frequently with normality.” Fuzzy boundaries among near diagnostic neighbors are common and not a sufficient excuse to collapse clinically valuable distinctions.
Carleton Erickson’s discussion of the degrees of severity with drug problems helps to illustrate this misunderstanding. He indicated there were mild, moderate and severe forms of both drug abuse and drug dependence. Most people don’t think in terms of severity with substance use problems. You either have a problem or you don’t; you either abuse drugs or you don’t. He then illustrated their relationship to drug-seeking behavior as follows.
|
Drug Abuse |
Drug Dependence |
Drug-Seeking |
|
Mild |
Little/None |
|
|
Moderate |
Some |
|
|
Severe |
Mild |
A Lot |
|
Moderate |
Even more |
|
|
Severe |
All the Time |
The overlap referred to by Frances occurs between severe drug abuse and mild drug dependence. The inability of psychiatric diagnosis to make a clear distinction here seems to have led to the decision to collapse the abuse and dependence diagnoses into one category in the DSM-5.
I think another overlap between drug abuse and drug dependence happens with regards to self-control. A distinction is necessary between self-control of thoughts, feelings and behavior when drinking and control of the drug intake itself. Any substance use can lead to a loss of self-control over an individual’s thoughts, feelings and behavior. When that loss of control results in recurrent, intermittent trouble, there is a drug abuse problem. The severity of this type of loss of self-control and the related intermittent trouble varies.
Not everyone who abuses a drug experiences the classic sense of losing of control over how much of the drug they use. A loss of control over drug intake—a continuous and compulsive pattern of use—is only evident within drug dependence. And again, the severity of this loss of control over drug intake varies. So I’d adopt Erickson’s degrees of severity with drug abuse and dependence problems as seen below.
|
Loss of Self-Control in Abuse |
Loss of Control over Drug Intake in Dependence |
|
Mild |
|
|
Moderate |
|
|
Severe |
Mild |
|
Moderate |
|
|
Severe |
A substance abuse problem with severe trouble related to loss of self-control may be indistinguishable from a substance dependence problem with mild loss of control over drug intake. Both people would look at their severe “trouble” and attribute it to drinking or drugging too much. Given an equal motivation to avoid further “trouble,” the substance abuser would likely have an easier time maintaining abstinence. Carleton Erickson said chemical dependence is not a “too much, too often, withdrawal” disease; it’s a “I can’t stop without help disease.” There is a pathological, compulsive pattern to substance use.
There does seem to be a “fuzzy boundary” between Substance Abuse and Substance Dependence. Nevertheless, the distinction still carries some clinical and diagnostic value. I agree with what Allen Frances said: “The change was radical, creates obvious harms, and provides no apparent benefit.” What should clinicians do? Frances suggested they simply ignore the DSM-5 change. He said it was appropriate and clinically preferable to continue making the distinction.
There is nothing sacred or official about the DSM-5 choices — I know because I made the choices for DSM-IV. The ICD coding system is official; the DSM codes are just one groups’ fallible adaptation of them. It is of great significance that the official coding in ICD-10-CM does not follow the DSM-5 decision to eliminate Substance Abuse. Instead, ICD-10-CM retains the DSM-IV terminology and continues to provide separate Substance Abuse and Substance Dependence codes for each of the major classes of substances.
The ICD-11 workgroup, currently in the final stage of development before field tests, will continue to separate Substance Dependence and Harmful Substance Use. The guidelines for dependence are revised and simplified into three diagnostic features: impaired control over substance use; increasing priority in life and physiological features. Severity qualifiers were suggested only for alcohol intoxication. They also introduced a new diagnostic category, with no equivalents in ICD-10 or DSM-5: single episode of harmful use. Frances commented:
The DSM-5 mistake thus places it out of line with ICD-10, ICD-11, previous DSM’s, and well established clinical practice. Clinicians remain truer both to clinical reality and to ICD coding when they ignore the new DSM-5 lumping of substance use disorders and instead continue to distinguish Substance Abuse from Substance Dependence. DSM’s are explicitly meant to be used only as guides, not worshiped as bibles. Clinicians are free to ignore DSM whenever it makes mistakes that go against clinical common sense and the International coding system.