
Repeating Past Mistakes

© kbuntu | 123rf.com
At 4:45 a.m. on September 1, 1939, 1.5 million German troops invaded Poland. Two days later Britain and France declared war on Germany and World War II had begun. This “blitzkrieg” strategy became a blueprint of how Hitler intended to wage war. Generally unknown, one of the key tools in the success of the German Wehrmacht was their use of a methamphetamine called Pervitin. The troops were literally on cloud nine about Pervitin, as were their commanders.
Reports from the front lines on the drug included the following glowing testimonies:
Everyone fresh and cheerful, excellent discipline. Slight euphoria and increased thirst for action. Mental encouragement, very stimulated. No accidents. Long-lasting effect.The feeling of hunger subsides. One particularly beneficial aspect is the appearance of a vigorous urge to work. The effect is so clear that it cannot be based on imagination.
Not surprisingly, addiction became a problem. In April and May of 1940 alone, the Nazis shipped 35 million units of Pervitin and similar medications to its troops. Troops at the front sent letters home begging for more Pervitin. “Everybody, from generals and their staffs to infantry captains and their troops, became dependent on methamphetamine.” A lieutenant colonel leading a Panzer division wrote the following in a report:
Pervitin was delivered officially before the start of the operation and distributed to the officers all the way down to the company commander for their own use and to be passed on to the troops below them with the clear instruction that it was to be used to keep them awake in the imminent operation. There was a clear order that the Panzer troop had to use Pervitin.
“Speed” or amphetamine is in ADHD medications like Adderall (amphetamine/dextroamphetamine), Vyvanse (lisdexamfetamine). Methylphenidate (Concerta, Ritalin, Daytrana) is their close chemical relative. By the way, don’t be fooled by the creative spelling done by Shire for Vyvanse: “lisdexamfetamine” instead of “lisdexamphetamine.” Writing for The Guardian, Alexander Zaitchik noted how the phonetic sleight-of-hand of Shire with Vyvanse and its aggressive marketing contributed to its success in getting the FDA to approve Vyvanse to treat “Binge Eating Disorder.”
The company’s neo-phoneticism is intended to put more distance between its new golden goose and the deep clinical literature on speed addiction, not to mention last century’s disastrous social experiment with widespread daily speed use, encouraged by doctors, to temper appetites and control anxiety.
What follows is a history of amphetamines gleaned primarily from two sources: a paper on Amphetamines from the Center for Substance Abuse Research (CESAR) of the University of Maryland and a 2008 article by Nicolas Rasmussen for the American Journal of Public Health, “America’s First Amphetamine Epidemic 1929-1971.”
Amphetamine was first synthesized by a German chemist in 1887, but its stimulant effects weren’t noticed until the early 1930s, when it was rediscovered by accident. The chemist was trying to make ephedrine, a decongestant and appetite suppressant. Branded as Benzedrine, amphetamine was marketed as an inhaler for nasal congestion by the pharmaceutical company, Smith, Kline & French starting in 1933. It didn’t take some people long to figure out how to use Benzedrine for its euphoric effect. They cracked the container open and swallowed the Benzedrine-coated paper strip or steeped it in coffee.
Its use grew rapidly as medical professionals recommended amphetamine for alcohol hangover, depression, narcolepsy, weight-loss, hyperactivity in children and morning sickness in pregnant women. “The use of amphetamine grew rapidly because it was inexpensive, readily available, had long lasting effects, and because medical professionals purported that amphetamine did not pose an addiction risk.” During World War II, amphetamines or methamphetamine (a derivative of amphetamine) were used by both Allied and Axis troops to increase their alertness and endurance, as well as to improve their mood.
By 1945, over 500,000 civilians were using amphetamine psychiatrically or for weight loss. Between 1945 and 1960 commercial competition drove amphetamine use higher. After a patent expired in 1949, the FDA estimated the production of amphetamine and methamphetamine rose almost 400% by 1952. By 1962, production of amphetamines was approaching 43 standard 10-mg doses per person. This compares to concerns with the 65 doses per year in the present decade that social critics of our cultures point to as evidence of the overuse of psychotropic medications.
The adverse effects of amphetamine were becoming more evident by 1960. Amphetamine psychosis had been known since the 1930s, but was initially attributed to the drug unmasking latent schizophrenia. This claim is eerily similar to current interpretations of antidepressant activation unmasking latent bipolar disorder, rather than being seen as an adverse side effect of antidepressant medication. There were also concerns that amphetamines were addictive. But this didn’t stop individuals like President John F. Kennedy from using regular injections of vitamins, hormones and 15 mg of methamphetamine to help maintain his image of youthful vigor.
Large quantities of amphetamines were dispensed in the 1960s directly by diet doctors and weight loss clinics. Calculations of amphetamine use and misuse in 1970 estimated that at least 9.7 million Americans had used the drugs in the past year. And of those 9.7 million users, 3.8 million do so for nonmedical reasons and 2.1 million of those abused the drugs. Rasmussen said this first amphetamine epidemic was iatrogenic, “created by the pharmaceutical industry and (mostly) well-meaning prescribers.” The current problem with the misuse of amphetamines has reached the peak of the original epidemic, namely about 3.8 million past-year nonmedical amphetamine users, with an estimated 320,000 of whom are addicted.
Parallel to this trend has been the surge in the legal supply of amphetamine-type ADHD medications such as Ritalin, Adderall and Vyvanse. American doctors, unlike those in other countries, have found it hard to resist prescribing these drugs. According to DEA production data, since 1995 medical consumption of these drugs has quintupled. In 2005, it exceeded the amphetamine consumption of 2.5 billion 10-mg amphetamine base units for medical use in 1969—compared to 2.6 billion base units in 2005. The following graph, taken from Rasmussen’s article, illustrates this increase. The data is based upon DEA production quotas and expressed as common dosage units of 10-mg amphetamine and 30-mg methylphenidate.
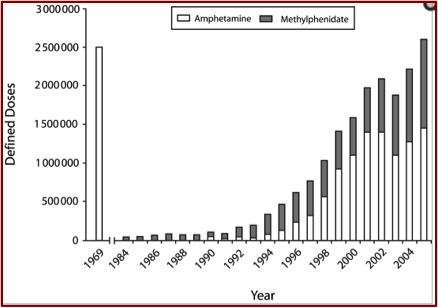 Rasmussen downplayed a causal connection between childhood stimulant treatment for ADHD and later nonmedical amphetamine consumption, but others don’t (See more on this below). However, he did think the wide distribution of ADHD stimulants, noted in the above graph, created a hazard. He cited data from a study that indicated 600,000 reported using stimulants other than methamphetamine nonmedically in the past month. So, “legally manufactured attention deficit medications like Adderall and Ritalin appear to be supplying frequent, and not just casual, misusers.”
Rasmussen downplayed a causal connection between childhood stimulant treatment for ADHD and later nonmedical amphetamine consumption, but others don’t (See more on this below). However, he did think the wide distribution of ADHD stimulants, noted in the above graph, created a hazard. He cited data from a study that indicated 600,000 reported using stimulants other than methamphetamine nonmedically in the past month. So, “legally manufactured attention deficit medications like Adderall and Ritalin appear to be supplying frequent, and not just casual, misusers.”
An analysis of stimulant abuse in recent national household drug surveys found that half of the 3.2 million reporting past-year nonmedical use of stimulants in the U.S. only used psychiatric stimulants. And 750,000 of those reported they had never used anything but attention deficit pharmaceuticals in their entire lives. “On this evidence alone, one can fairly describe the high production and prescription rates of these medications as a public health menace of great significance.”
Another problem is the widespread acceptance of prescription amphetamines as a legal and relatively harmless drug that can be given to small children. Rasmussen said it is difficult to make a convincing case that the same drug is harmful if used nonmedically. Therefore he concluded any attempt to deal harshly with methamphetamine users today in the name epidemic control, without touching medical stimulant production and prescription was practically impossible and hypocritical.
There is some evidence of a connection between childhood stimulant treatment and later abuse or use of stimulants. See “ADHD: An Imbalance of Fire Over Water or a Case of the Fidgets?” on this website for a discussion of the association of addiction and ADHD medications as well as other adverse effects.
Nadine Lambert did a longitudinal study of ADHD children and normal controls. Her participants were followed through their childhood and adolescence and then evaluated three times as young adults. “ADHD was also significantly associated with amphetamine dependence.” However, being diagnosed with ADHD did not increase the odds of lifetime use of stimulants. She found that treatment with stimulants increased the odds of lifetime use of amphetamine and cocaine/amphetamines.
Commenting on Lambert’s findings in Brain Disabling Treatments in Psychiatry, Peter Breggin said:
It is not ADHD but the treatment for ADHD that puts children at risk for future drug abuse. This conclusion is entirely consistent with the fact that animals and humans cross addict to Ritalin, amphetamine and cocaine and that exposure to Ritalin in young animals causes permanent changes in the brain.
Hitler and his generals wanted victory at any cost and Pervitin (methamaphetamine), was part of that solution. German pilots called it “pilot’s chocolate”; soldiers on the front called it “Panzerschokolade” or “tank chocolate.” But towards the end of WW II, Vice Admiral Hellmuth asked German pharmacologists to develop a miracle drug. They had a wonder drug with Pervitin, but now they needed a miracle drug. So Gehard Orxzechowski synthesized D-IX. It was supposed to keep soldiers ready for battle even when they were asked, “to continue beyond what was considered normal.” It contained 5 mm of cocaine, 3mm of Pervintin and 5mm of morphine. It seems it was a good thing the war ended before they could distribute it widely to their troops.
We have a lesson to learn from the German Wehrmacht’s failure to make a better, smarter, stronger soldier through chemicals. The American war on drugs needs to recognize its greatest casualties are now coming from within—as with ADHD medications. And I think we need to reflect on the words of George Santayana in The Life of Reason: “Those who cannot remember the past are condemned to repeat it.”