
The Dragon Threat

© Linda Bucklin | 123rf.com
The DEA released its updated “National Heroin Threat Assessment Summary” on June 27, 2016 and the news is not good. Chuck Rosenberg of the DEA called the death and destruction from heroin and opioids “unprecedented and horrific.” The number of users, treatment admissions, overdose deaths, seizures from heroin traffickers all increased since the 2015 Summary. The increased demand and use of heroin is being driven by greater availability of heroin in the U.S. and prescription opioid users switching to heroin because it’s cheaper. “The problem is enormous and growing, and all of our citizens need to wake up to these facts.”
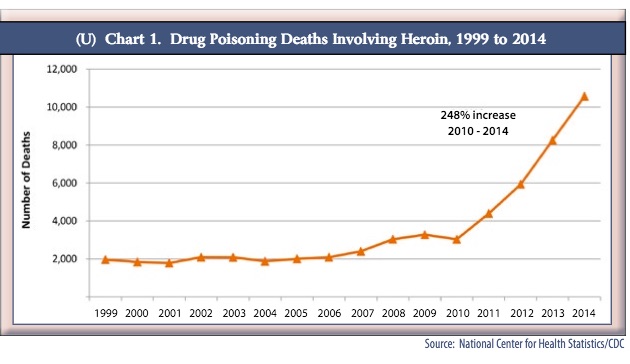
There were three big takeaways in the 2016 Summary: 1) the number of people currently using heroin almost tripled between 2007 and 2014. 2) Deaths due to heroin more than tripled between 2010 and 2014. 3) Deaths due to synthetic opioids, like fentanyl, increased 79% between 2013 and 2014. You can access a pdf of the full report here.
In 2014, 10,574 American died from heroin-related overdoses. Geographic areas of the country particularly hard hit are in the Northeast and the Midwest. See Map 2 in the 2016 DEA Summary. Not surprisingly, availability levels are the highest in these areas as well. Possible reasons for the increase in overdoses and deaths include: more heroin users, especially those who are new to heroin, who are young and inexperienced; the higher purity of heroin found in certain areas and the use of adulterants like fentanyl.
Twenty to thirty years ago, the average retail-level purity of heroin available in the U.S. was about 10%. By 1999, the average purity was 40%. While the purity increased, the price decreased. The average price per gram in 1981 was $3,260 in 2012 US dollars. By 1999, the price for a gram of heroin had dropped to $622. Heroin prices have remained low since then. With an increase in purity, heroin can be snorted or smoked, which broadens its appeal. “Many people who would never consider injecting a drug were introduced to heroin by inhalation.”
Beginning in late 2013, several states started reporting overdose death due to fentanyl and acetyl-fentanyl. There were 5,544 reported synthetic-opioid-related deaths in 2014. But the DEA speculated it was much higher because of a lack of standardization in reporting; and because coroners and state crime labs don’t initially test for fentanyl or its analogs unless they have a reason to do so. The eastern U.S. is the area most effected by this, because white powder heroin from South America predominates. Fentanyl, also a white powder, is mixed with heroin or sold disguised as white powder heroin. The following chart is from the 2016 DEA Summary.
 The Mississippi River has historically been a geographic dividing line with Mexican, “black tar” and brown powder heroin more common west of the Mississippi and white powder heroin, now supplied from South America, common east of the Mississippi. But that is changing. Mexican traffickers are making inroads into major eastern cities. Mexican organizations are now the most prominent wholesale-level traffickers of heroin in Chicago, New Jersey, Philadelphia, and Washington DC. Increased trafficking of Mexican heroin means more heroin is entering the U.S. across the Southwest border from Mexico. Black tar heroin is popping up more frequently in the Northeast, although it still comprises a small percentage of the heroin seized.
The Mississippi River has historically been a geographic dividing line with Mexican, “black tar” and brown powder heroin more common west of the Mississippi and white powder heroin, now supplied from South America, common east of the Mississippi. But that is changing. Mexican traffickers are making inroads into major eastern cities. Mexican organizations are now the most prominent wholesale-level traffickers of heroin in Chicago, New Jersey, Philadelphia, and Washington DC. Increased trafficking of Mexican heroin means more heroin is entering the U.S. across the Southwest border from Mexico. Black tar heroin is popping up more frequently in the Northeast, although it still comprises a small percentage of the heroin seized.
Mexican traffickers have taken a larger role in the U.S. heroin market, increasing their heroin production and pushing into eastern U.S. markets that for the past two decades were supplied by Colombian traffickers. This is notable because Mexican traffickers control established transportation and distribution infrastructures that allow them to reliably supply markets throughout the United States
The DEA also noted the increase in counterfeit prescription pills, many which contain deadly amounts of fentanyl. Small-scale local drug entrepreneurs can buy the materials and equipment to produce the counterfeit drugs online and set up their own operation, ala Breaking Bad. “Fentanyl pill press operations have been identified in the United States, Canada, and Mexico, indicating a vast expansion of the traditional illicit fentanyl market.” Oxycodone and other opioid painkillers are the main counterfeited medications, but traffickers are also packaging fentanyl as Xanax and other benzodiazepines. See “Buyer Beware Drugs” for more information.
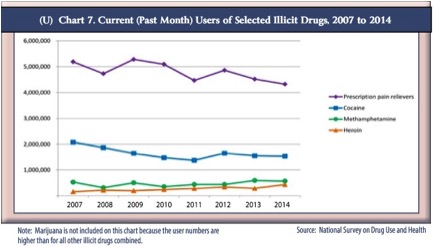
When comparing heroin use to other drugs in the U.S., we find that the population of heroin users is slightly smaller than the estimated population of methamphetamine users and significantly smaller than individuals reporting current cocaine use. However, the number of individuals reporting current use of prescription pain relievers non-medically was about TEN TIMES the size of heroin users. So although a rather small percentage of prescription drug abusers (4%) will try heroin, this represents a significant increase in the number of heroin users because the size of the prescription drug abuse population is so much larger. See the following chart taken from the 2016 DEA Summary.
 Behind all these statistics are real people, some living and some now dead. And despite all the law enforcement efforts over the past several decades, the problem seems to be getting worse. So two federal law enforcement agencies decided to combine their efforts and try a different tactic. They thought they’d try to address the problem from the demand side instead of the supply side.
Behind all these statistics are real people, some living and some now dead. And despite all the law enforcement efforts over the past several decades, the problem seems to be getting worse. So two federal law enforcement agencies decided to combine their efforts and try a different tactic. They thought they’d try to address the problem from the demand side instead of the supply side.
Back in February the FBI and DEA released a documentary film addressing the growing epidemic of prescription drug and heroin abuse. “Chasing the Dragon: The Life of an Opiate Addict” is intended as an educational film for high school and above. Educational materials have had mixed effectiveness with decreasing drug usage. But the value of this film is in its portrayal of the real people who chased the dragon and became part of the above statistics. You can watch the film here.
