David and the Uncircumcised Philistine

© tupungato | 123rf.com.
Between 2007 and 2013 Yosef Garfinkel of the Hebrew University of Jerusalem and two others led excavations at a site in the Elah Valley known as Khirbet Qeiyfa. Among the artifacts found there is perhaps the oldest inscription written in Hebrew. There also was a cultic stone shrine decorated with architectural elements that echo biblical descriptions of Solomon’s Temple and his palace in Jerusalem. Carbon dating places the city’s existence around the 11th and 10th century BC, at the beginning of the Kingdom of Israel. Perhaps most intriguingly, the site is located on the Philistine and Judean border “in the area that has been identified as the location of the battle between David and Goliath.”
In September of 2016 the Bible Lands Museum in Jerusalem opened an exhibition focused on the archeological discoveries at Khirbet Qeiyfa called “In the Valley of David and Goliath.” The archaeologists only realized during their second season of excavations that their fortified town “perfectly fit the descriptions of the Biblical town of Shaarayim.” The Hebrew name of the town means “two gates,” which is what was uncovered during the excavations; two gates. You can watch a short video about the exhibition here. There is an article about the Khirbet Qeiyfa archeological site here.
The geographical location of the town also fits right in line with the Biblical depiction of Shaarayim, mentioned in the context of the aftermath of the battle between David and Goliath when the Philistines “fell on the way to Shaarayim.” The town is also mentioned in the book of Joshua as being situated near Socho and Azeka, two archaeological sites surrounding Khirbet Qeiyafa.
The story of David and Goliath is the classic biblical tale of the big bully getting his comeuppance from the little guy. In his commentary on 1 Samuel, Robert Bergen said in Western culture it has become the primary historical metaphor for “describing any individual or group who overcomes seemingly insurmountable odds to defeat an oppressor.” In 1960, the story became a feature length Italian film, where Orson Welles, no less, played King Saul. The feature length movie is available on Amazon Prime and YouTube. There is even a TED Talk by Malcom Gladwell that reviews the biblical account, “The Unheard Story of David and Goliath.”
Gladwell’s account of David and Goliath tends to minimize Goliath’s threat as an opponent to David, while drawing out the danger David and his sling posed to Goliath. According to Gladwell, Goliath was only 6’ 9’’ tall. He referred to Goliath’s shield bearer as a young boy or attendant who led him by the hand. And he cited medical speculation that Goliath’s 6’ 9” height was the result of acromegaly, a condition caused by a benign tumor on the pituitary gland that causes an overproduction of growth hormone. The distinct side effects from acromegaly were then used to explain other aspects of the David and Goliath encounter. Later we’ll look at biblical and extra biblical evidence that challenges this portrayal of Goliath, but first let’s look at his assessment of David and his choice of weapons.
David rejects the offered use of Saul’s armor, instead choosing to take his shepherd’s staff, his sling and five smooth stones. Gladwell noted where soldiers of that time would fight with slings. He speculated that when David released his rock, it was traveling 35 meters per second; faster than a baseball thrown by the best pitchers. “If you do the calculations on the ballistics, on the stopping power of the rock fired from David’s sling, it’s roughly equal to the stopping power of a [.45 caliber] handgun.”
This made the sling a very powerful weapon, one that some have called “the gun” of the ancient world. Sling stones excavated at the main gate of the city of Lachish (pictured below in The British Museum) were as big as tennis balls. Slingers are known to be accurate enough to hit birds in flight; and to hit, maim or kill a target up to 200 yards away. “If you go back over the history of ancient warfare, you will find time and time again that slingers were the decisive factor against infantry in one kind of battle or another.”
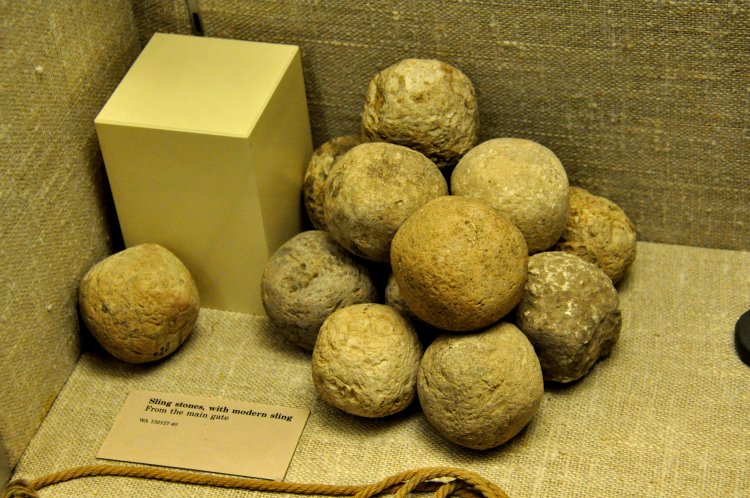
photo by: Osama Shukir Muhammed Amin; licensed under Creative Commons: Attribution-NonCommercial-ShareAlike
Goliath’s weapons and armor could have weighed more than 150 pounds (His armor alone weighed 126 pounds). His combat gear was designed for close combat. The weight of his spearhead was around fifteen pounds; too heavy and awkward for throwing. He was covered from head to toe in metal. He wore a bronze helmet; armor; bronze greaves (knee and shin protection). He had a bronze javelin (more likely a scimitar) slung between his shoulders. And he had a full body shield or ṣinnâ carried by a shield bearer, who went ahead of him. The assumption by Gladwell of Goliath being led by a youth is inaccurate.
Without Saul’s armor, David would have had greater mobility. This and the fact that Goliath was outfitted for close combat explain his invitation for David to “come to him” in 1 Samuel 17:44. David ran quickly towards Goliath after they exchanged insults because he wasn’t afraid, for two reasons. First and foremost, he knew that the Lord would deliver him (1 Samuel 17:37). Second, he knew from past experience that he had killed both lions and bears. Based on David’s future tactical skills in warfare, I would speculate that he realized Goliath’s vulnerability to attack by a skilled slinger, which he knew himself to be.
Goliath really was huge. He was 9’ 9’’ tall; not 6’ 9” tall. The different reported heights are due to the six cubit height recorded in 1 Samuel 17:4 versus the recorded height of four cubits in the Codex Vaticanus (an important Greek manuscript of the Old and New Testaments) and Josephus, as well as a copy of the Septuagint. Bergen suggested the shorter figure is an emendation to the text by a pious copyist to increase the text’s credibility. However, a smaller Goliath then creates problems for the bulk of his combat gear, like a 15-pound spearhead.
There are several other biblical references to giants. The twelve spies reported to the Israelites there were Anakim in the land, a people “greater and taller” than they were (Numbers 13:28; Deuteronomy 1:28). After wandering forty years in the wilderness, Moses told the Israelites they would confront the Anakim when they crossed the Jordan into Canaan (Deuteronomy 9:2). Joshua defeated the Anakim from the hill country of Judah, destroying them and their cities. But some remained in the Philistine cities of Gaza, Gath and Ashdod (Joshua 11:21-23). They were driven from Hebron by Caleb (Joshua 14:12-15).
The Anakim were believed to be the descendants of Anak and dwelt in the region around Hebron. Their name means “people of the necklace.” R. K. Harrison noted where the 18th century BC Egyptian Execration Texts seemed to point to a tribe named Anak. Referring to the Egyptian Execration Texts in Space and Time in the Religious Life of the Near East, Nicholas Wyatt described how the Egyptians performed a curse ritual on their enemies in Canaan, including the rulers of Iy-Anaq. The IVP Bible Background Commentary: Old Testament reported that Papyrus Anastasi I, a 13th century BC document, referred to fierce warriors that were seven to nine feet tall. Josephus described how Caleb conquered Hebron, killing all its inhabitants, who were a race of giants:
For which reason they removed their camp to Hebron; and when they had taken it, they slew all the inhabitants. There were till then left the race of giants, who had bodies so large, and countenances so entirely different from other men, that they were surprising to the sight, and terrible to the hearing. The bones of these men are still shown to this very day, unlike to any creditable relations of other men.
The IVP Bible Background Commentary: Old Testament also reported that two female skeletons about seven feet tall from the 12th century BC were found at Tell es-Sa’ideyeh in Transjordan. However, Jonathan Tubb, who was in charge of the excavation of Tell es-Sa’ideyeh, said “no such skeletons were found there.”
Moderns are distant enough from Josephus and the biblical reports of the Anakim and Goliath to be skeptical that humans as tall as nine feet once lived on the earth. The confirmed proof of seven or nine foot skeletons has so far been lacking support. But there is a tantalizing suggestion that there was such evidence at one time. In On the Resurrection of the Flesh, as Tertullian speculated on the meaning of New Testament texts on the resurrection from the dead, he made an aside comment about giants: “There are the carcasses of the giants of old time; it will be obvious enough that they are not absolutely decayed, for their bony frames are still extant.”
The archaeological evidence of an ancient race or tribe of giants, of Anakim, is still missing. Perhaps it will never be found and speculation on the veracity of the story of David and Goliath will continue. Biblical scholars have voiced a variety of concerns with it, including the differences between the Masoretic text (Goliath 9’ 9’’ tall) and the Septuigint (Goliath 6’ 9’’) noted above. Another concern is with 2 Samuel 21:19, where it says Elhanan struck down Goliath. Complicating the issue further, is 1 Chronicles 20:5, which says Elhanan struck down Lahmi, the brother of Goliath. The best explanation seems to be that 2 Samuel 21:19 is a copyist error from pre-Christian times. 1 Chronicles 20:5 preserves the correct and accurate reading.
Undoubtedly, the writer of 1 Samuel wanted to impress the story of David and Goliath onto the minds of his readers. Robert Bergen noted several narrative techniques that support this conjecture. First is the length of the account, 912 words in Hebrew. That is longer than any other single Davidic battle narrative. Second, there are more quotations (22) than there are in other stories. The longest quote in 1, 2 Samuel is by Goliath in 1 Samuel 17:8-9.
There are also details normally missing from similar narratives. We know the pieces and weight of Goliath’s armor, the number of cheeses and loaves of bread David brings from his father, how David selected his sling stones, and even that he drew Goliath’s sword from its sheath to kill him and cut off his head. “These details force the reader to ponder the narrative after its reading and thus make the story more memorable and more likely to be studied further.”
Bergen also noted the passage in 1 Samuel 17 was the longest description of military attire in the Old Testament. “Goliath’s physical stature, armor, weaponry, and shield bearer must have made him appear invincible.” All these external advantages suggest that chapter 17 was at least partly intended as an object lesson for the previous chapter in verse 16:7, when the Lord told Samuel to not look on the outward appearance of Eliab, David’s brother. Outwardly Goliath was the premier warrior. And yet, he was overcome and killed by the young shepherd David.
Another contrast exists between the physical stature of Saul and David. Saul was described as being taller than any of the people. He was literally head and shoulders above them. When Samuel presented Saul to the people he said: “Do you see him whom the Lord has chosen? There is none like him among all the people” (1 Samuel 10:23-24). David was just a youth (1 Samuel 17:33). He could not wear Saul’s armor when he went to challenge Goliath, because he had not tested it; he wasn’t used to it (1 Samuel 17:39). Yet David brought about the victory in the Valley of Elah that Saul, a proven warrior and leader, could not. The message of the passage is to simply not trust in outward appearances; trust God instead.